The document outlines Afghanistan's 2021 National Emergency Action Plan for polio eradication. Key points include:
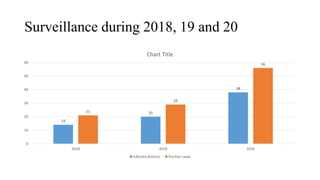
- Afghanistan reported 56 polio cases in 2020 as transmission spread to new areas. Barriers to access and campaign quality pose major challenges.
- The plan's goals are to stop transmission in the South and East and respond rapidly to any new outbreaks. Strategic interventions include vaccination campaigns, improving quality in accessible areas, and maximizing reach in inaccessible regions.
- It focuses on high-risk provinces and districts, prioritizing improving frontline workers and training, strengthening surveillance, and using communication strategies to improve vaccine acceptance. Convergence with EPI and integrated service delivery aims to build population immunity