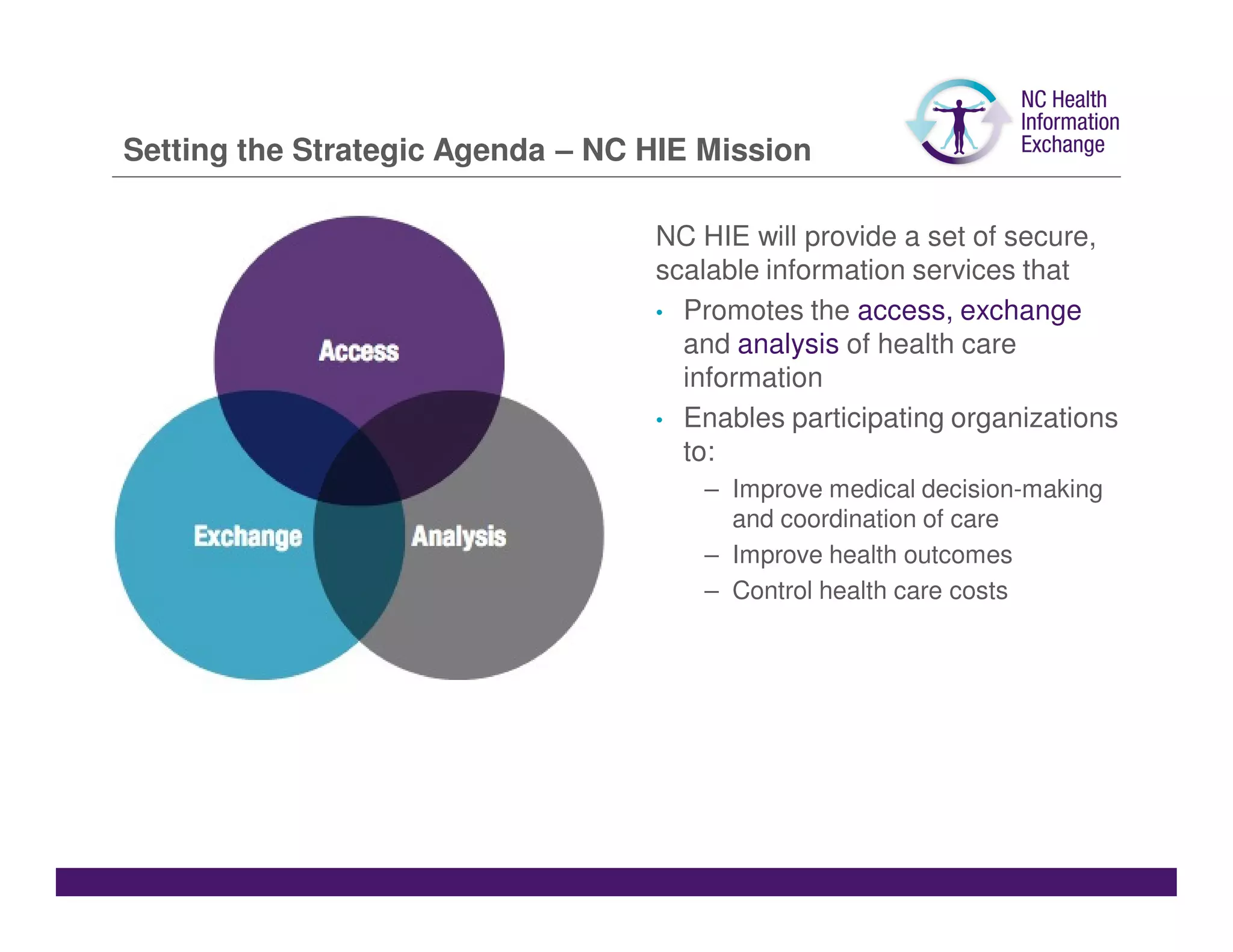
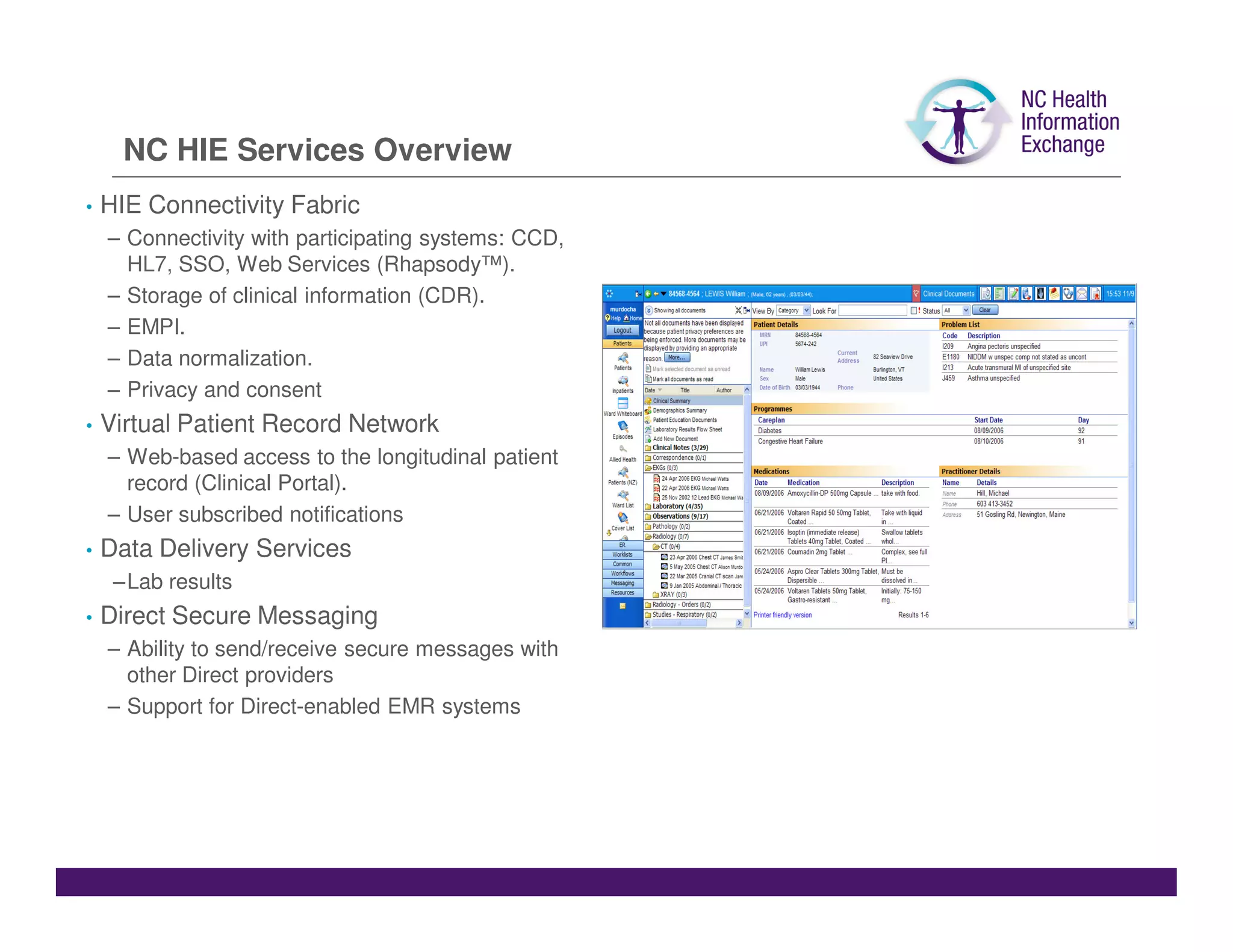
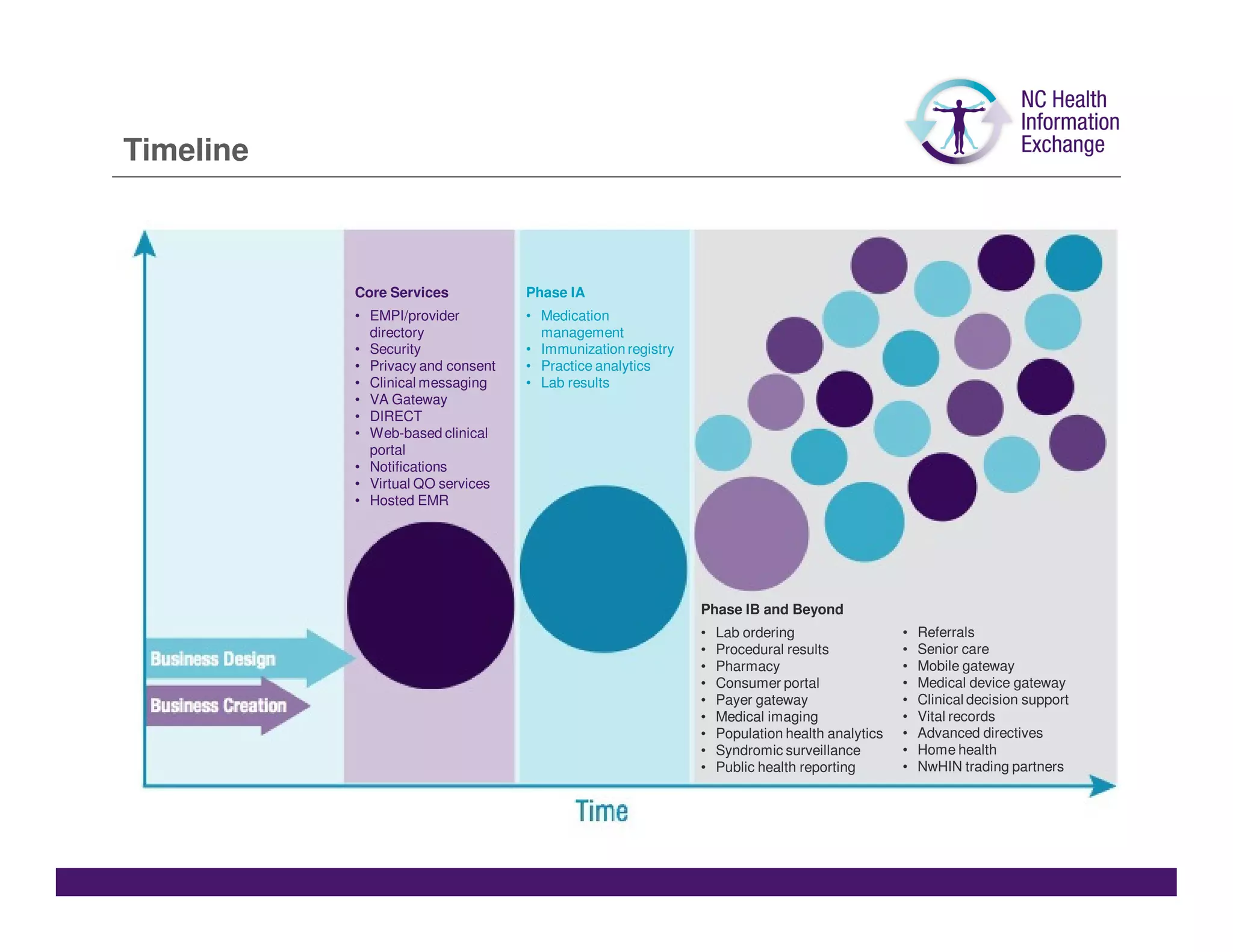
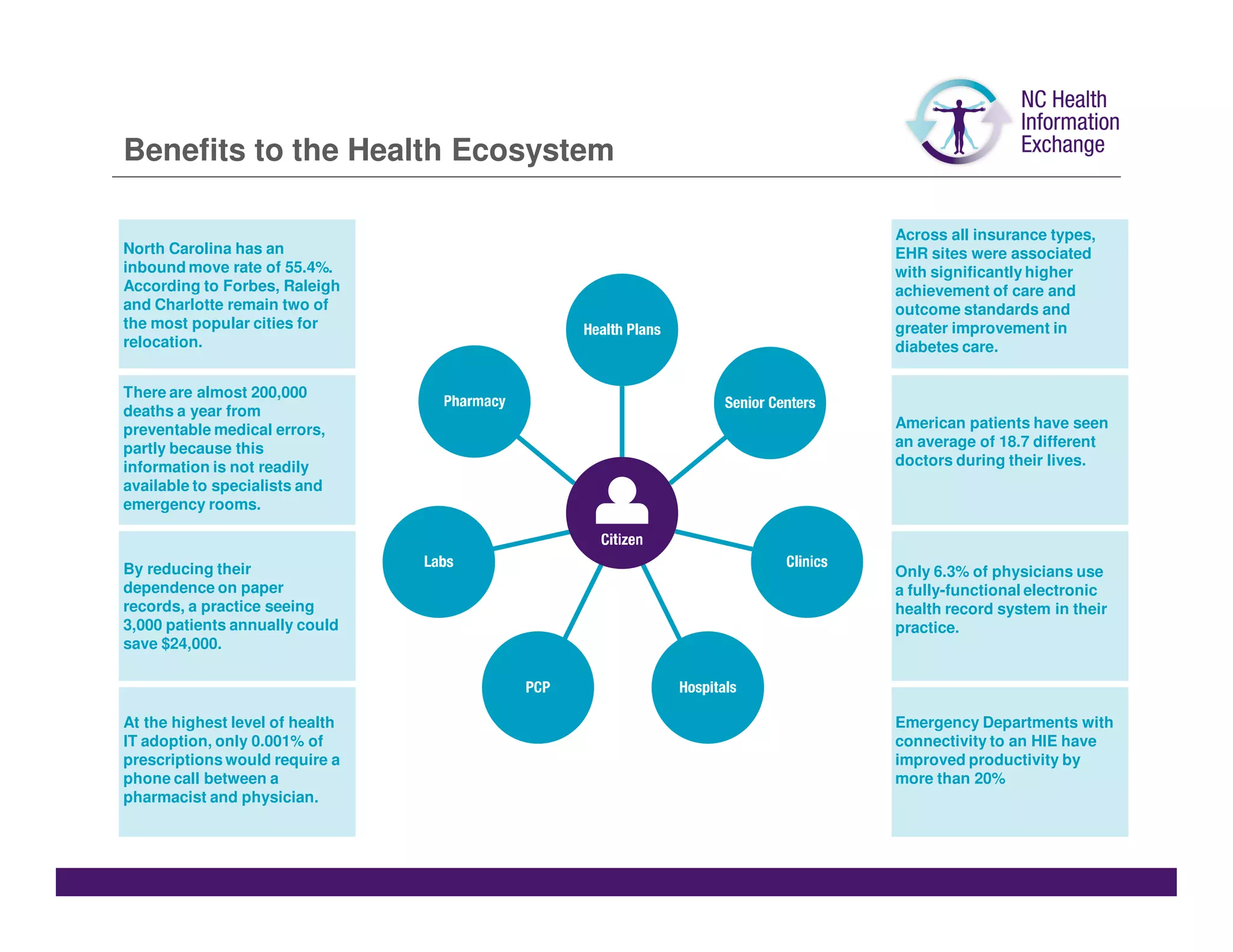
The document summarizes a presentation given by Jeff Miller about the North Carolina Health Information Exchange (NC HIE). The NC HIE is a nonprofit organization established in 2010 to facilitate the secure exchange of health information across the state. It has a 25-member board of directors and four workgroups focused on clinical operations, governance, finance, and legal/policy issues. The goals of the NC HIE are to improve medical decision making, care coordination, health outcomes, and reduce costs by enabling the access and exchange of health data. The NC HIE provides various services like connectivity with participating systems, a clinical portal, secure messaging, and will expand offerings over time. Benefits of the NC HIE include better, safer, more