Download to read offline





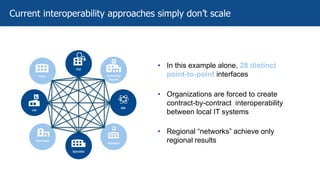
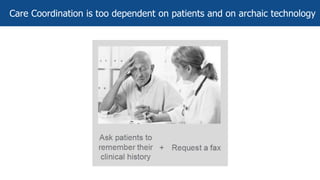
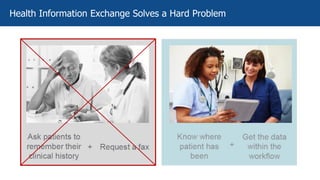

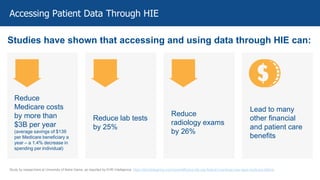
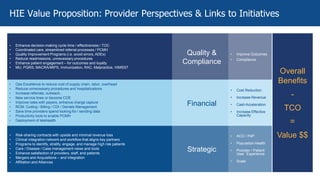


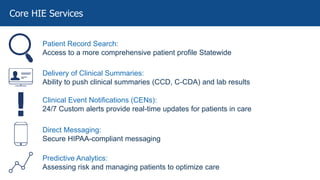
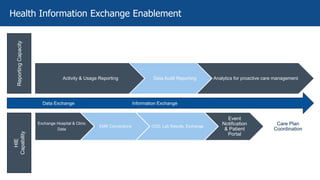
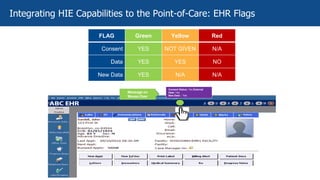

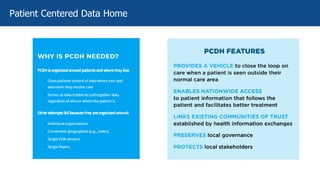
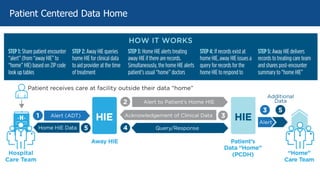
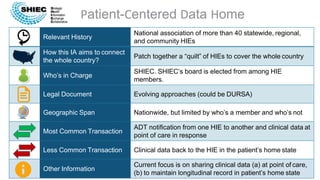
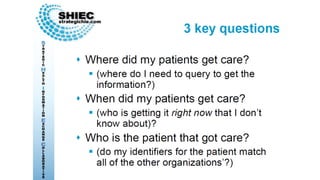
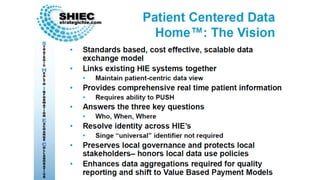




The document discusses best practices for enabling Health Information Exchange (HIE) and integrating its capabilities into Electronic Health Record (EHR) workflows, emphasizing the necessity of HIE in delivering value-based care and enhancing patient outcomes. It outlines various use cases, benefits, and challenges of HIE, alongside the roles of organizations like the Strategic Health Information Exchange Collaborative (SHIEC) and the Patient-Centered Data Home (PCDH). It highlights the importance of interoperability, care coordination, and leveraging data analytics to manage healthcare costs and improve patient care efficiency.











































































