Downloaded 41 times


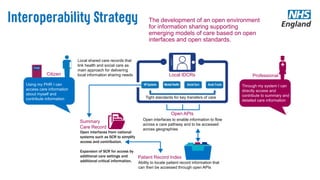


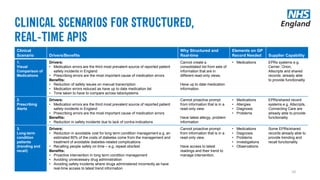
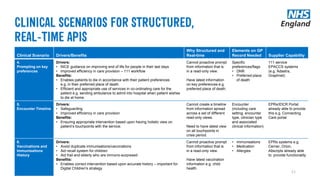
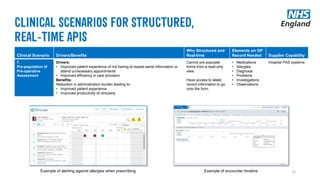



1) The document discusses developing an open environment for information sharing to support new models of care through open interfaces, standards, and APIs. 2) It outlines current priorities like using NHS numbers as primary identifiers and electronically sharing discharge summaries. 3) The goal is to open up key national systems like the Summary Care Record through structured APIs to allow access and contribution of important clinical information based on industry standards.
























































































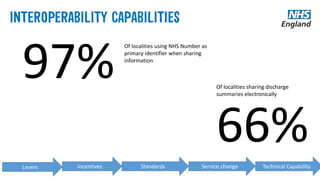
![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








