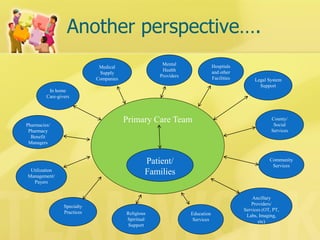
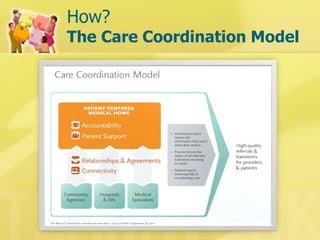
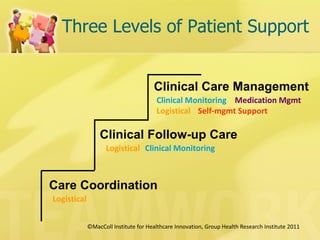
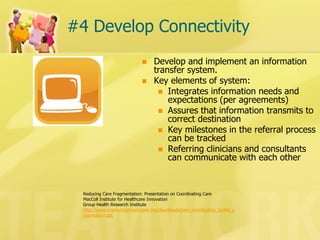
This document discusses care coordination in the medical home. It defines care coordination as organizing patient care activities between multiple participants to facilitate appropriate healthcare delivery. Effective care coordination involves numerous participants exchanging information and integrating care activities. The care coordination model aims to deliver the right services, in the right order and setting. Key elements of the model include assuming accountability for coordination, providing patient support, developing relationships and agreements with other providers, and improving connectivity through information sharing.




























![[1] documentation and reporting](https://cdn.slidesharecdn.com/ss_thumbnails/1documentationandreporting-150205213856-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)












































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









