Download to read offline
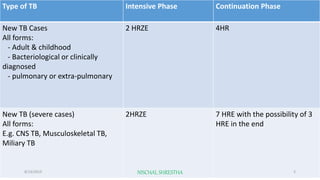
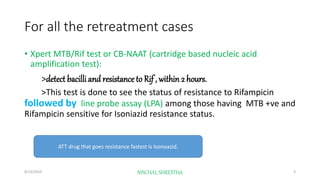
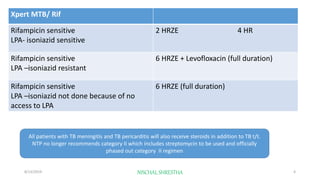
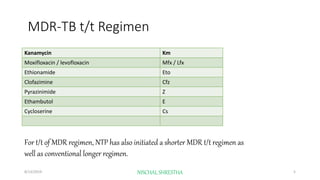
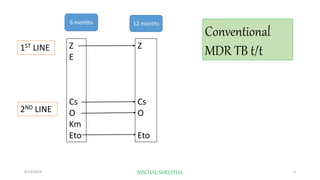
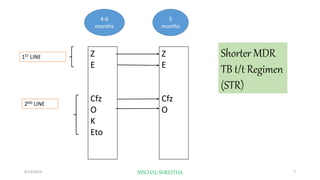

The document details the tuberculosis (TB) treatment regimens used in Nepal for the fiscal year 2074/2075, emphasizing both new and retreatment cases, including the phases of treatment and specific tests for drug resistance. It outlines the categorization of drugs, including the phasing out of certain regimens and the introduction of shorter and longer MDR-TB treatment regimens. Additionally, it highlights the use of novel drugs like bedaquiline for complex TB cases.































![Updated Part -3 Management of TB.. DR. Kiran G. Piparva 2020 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/updatedpart-3managementoftb-220926163033-9d05f002-thumbnail.jpg?width=640&height=640&fit=bounds)















































