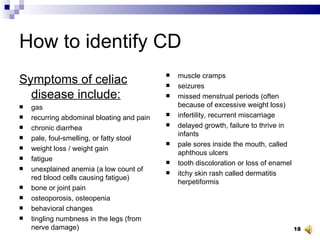
1) Celiac disease is an autoimmune disorder where the ingestion of gluten leads to damage in the small intestine. It affects approximately 1 in 100-150 people worldwide.
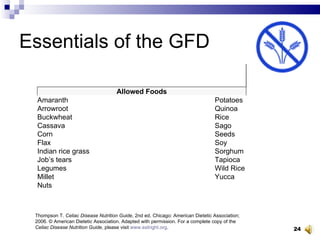
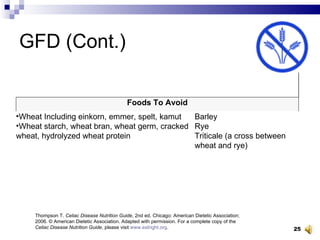
2) Left untreated, celiac disease can cause nutrient deficiencies, bone loss, fatigue and other issues. The only treatment is a strict lifelong gluten-free diet.
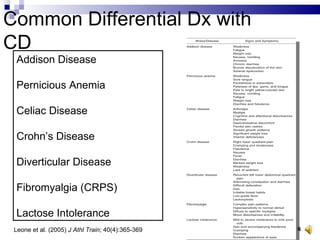
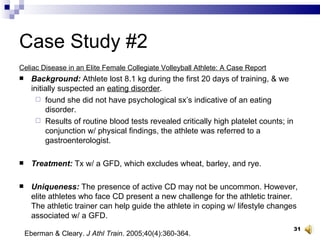
3) The document discusses two case studies of college athletes diagnosed with celiac disease and how identifying and treating the condition helped improve their athletic performance and health.


![Resources Celiac Disease Awareness Campaign National Digestive Diseases Information Clearinghouse 2 Information Way Bethesda, MD 20892–3570 Phone: 1–800–891–5389 Fax: 703–738–4929 Email: [email_address] Internet: www.celiac.nih.gov](https://image.slidesharecdn.com/nata2008celiacathleticsleone-1232392928020715-1/85/Nata-2008-Celiac-Athletics-Leone-38-320.jpg)
![American Celiac Society P.O. Box 23455 New Orleans, LA 70183–0455 Phone: 504–737–3293 Email: [email_address] Internet: www.americanceliacsociety.org](https://image.slidesharecdn.com/nata2008celiacathleticsleone-1232392928020715-1/85/Nata-2008-Celiac-Athletics-Leone-39-320.jpg)
![American Dietetic Association 120 South Riverside Plaza, Suite 2000 Chicago, IL 60606–6995 Phone: 1–800–877–1600 Email: [email_address] Internet: www.eatright.org](https://image.slidesharecdn.com/nata2008celiacathleticsleone-1232392928020715-1/85/Nata-2008-Celiac-Athletics-Leone-40-320.jpg)
![Celiac Disease Foundation 13251 Ventura Boulevard, #1 Studio City, CA 91604 Phone: 818–990–2354 Fax: 818–990–2379 Email: [email_address] Internet: www.celiac.org](https://image.slidesharecdn.com/nata2008celiacathleticsleone-1232392928020715-1/85/Nata-2008-Celiac-Athletics-Leone-41-320.jpg)
![Celiac Sprue Association/USA Inc. P.O. Box 31700 Omaha, NE 68131–0700 Phone: 1–877–CSA–4CSA (272–4272) Fax: 402–558–1347 Email: [email_address] Internet: www.csaceliacs.org](https://image.slidesharecdn.com/nata2008celiacathleticsleone-1232392928020715-1/85/Nata-2008-Celiac-Athletics-Leone-42-320.jpg)
![Gluten Intolerance Group of North America 31214 124th Avenue SE Auburn, WA 98092 Phone: 253–833–6655 Fax: 253–833–6675 Email: [email_address] Internet: www.gluten.net](https://image.slidesharecdn.com/nata2008celiacathleticsleone-1232392928020715-1/85/Nata-2008-Celiac-Athletics-Leone-43-320.jpg)
![National Foundation for Celiac Awareness P.O. Box 544 Ambler, PA 19002 Phone: 215–325–1306 Email: [email_address] Internet: www.celiaccentral.org](https://image.slidesharecdn.com/nata2008celiacathleticsleone-1232392928020715-1/85/Nata-2008-Celiac-Athletics-Leone-44-320.jpg)