Downloaded 18 times















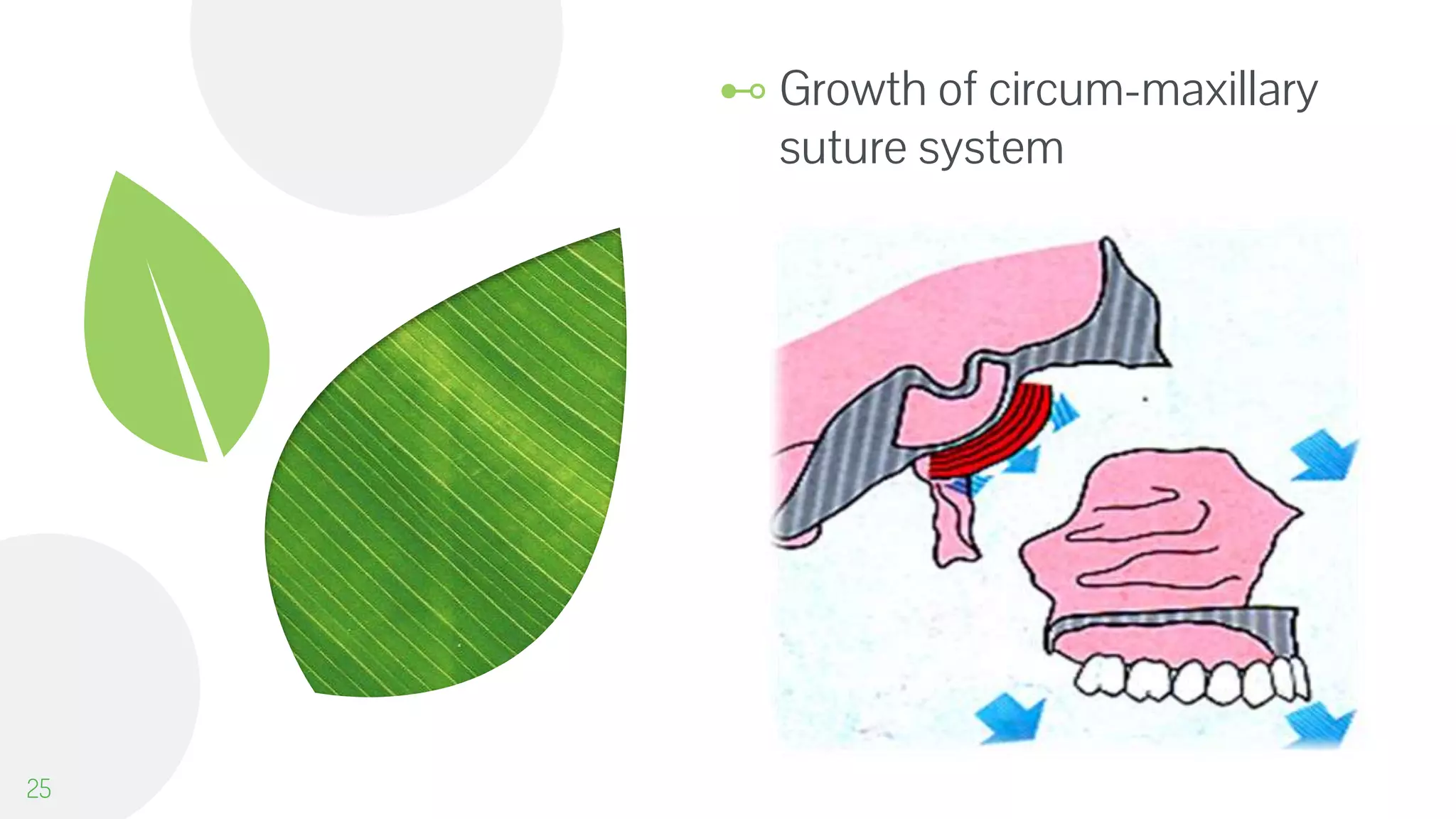



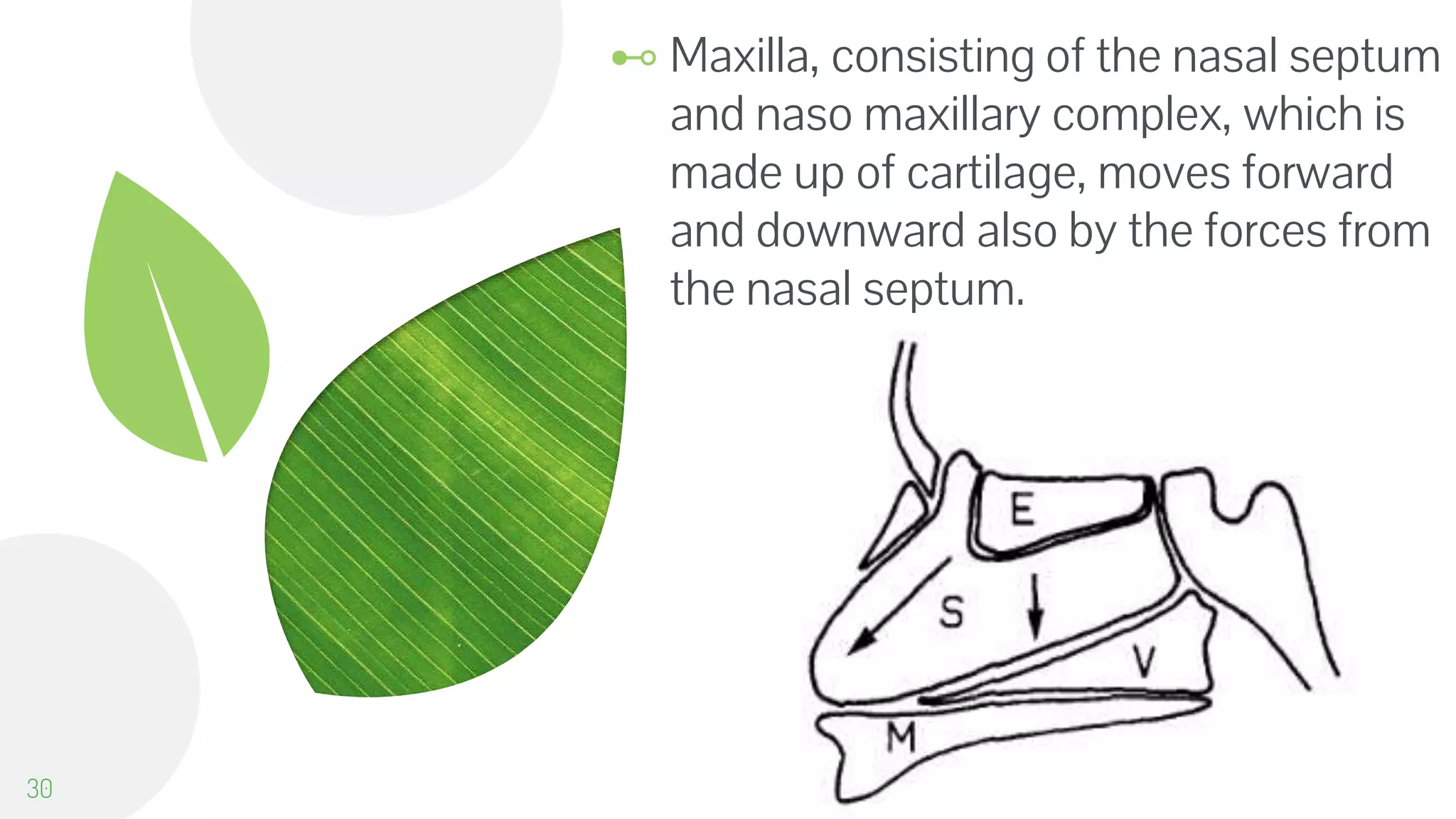
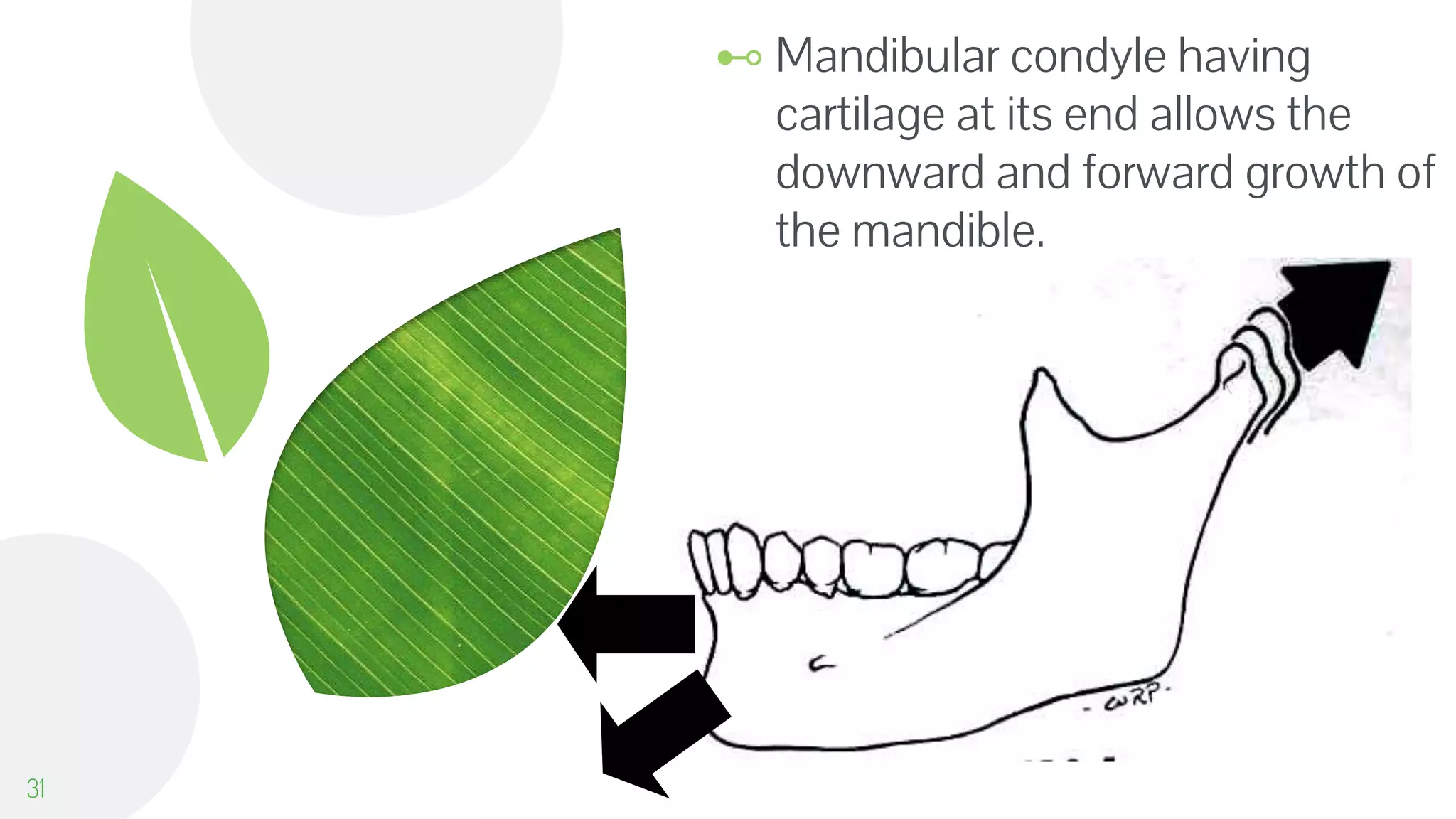









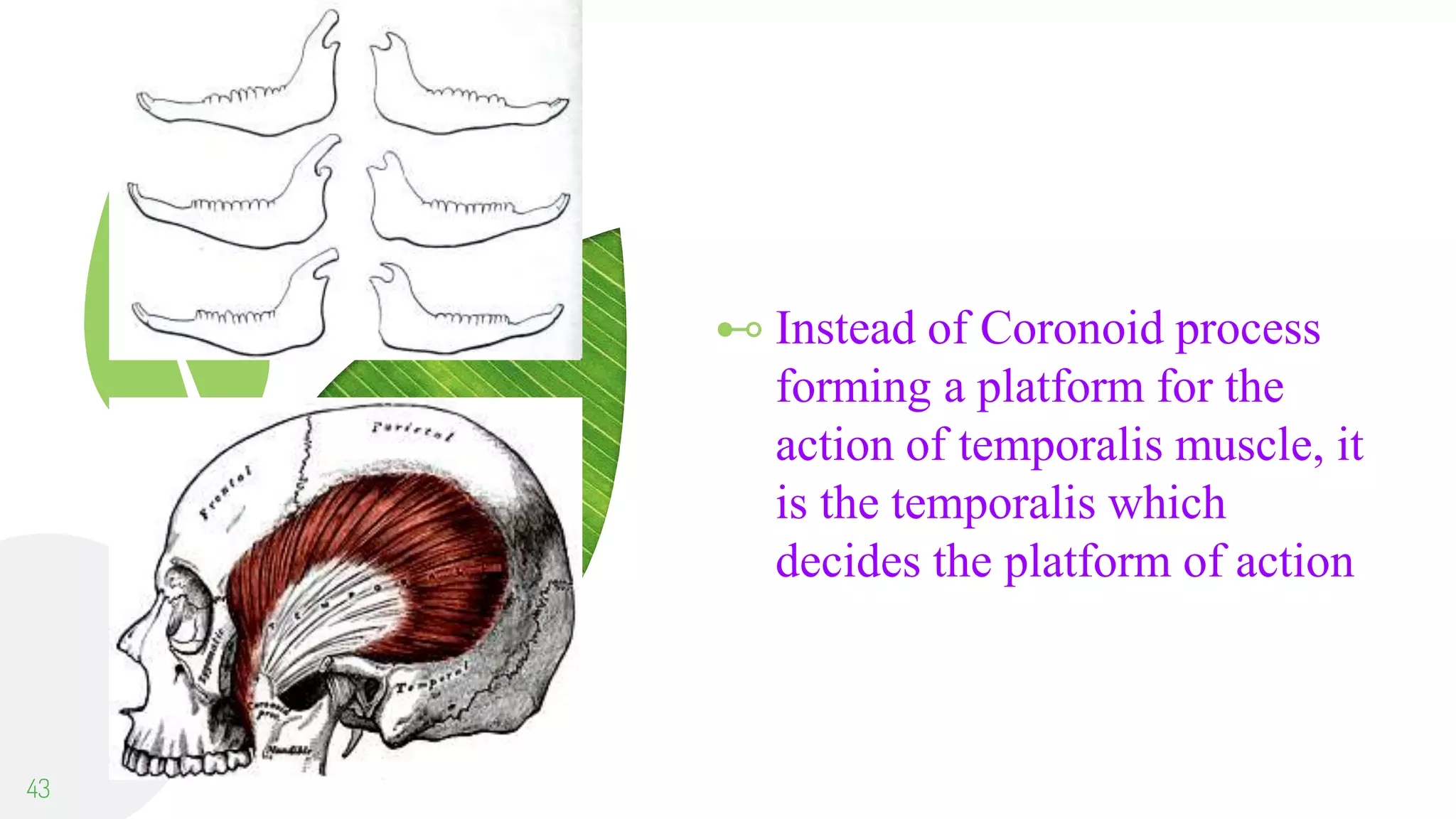



























This document provides an overview of several theories of craniofacial growth and development: - The bone remodeling theory proposed growth occurs through bone remodeling at surfaces. It did not explain roles of sutures or cartilages. - The genetic theory stated genes determine overall growth patterns but did not prove this assumption. - The sutural dominance theory proposed sutures are the primary growth determinants through expansion forces. However, growth still occurs without sutures. - The cartilaginous theory claimed cartilage, not bone, is responsible for growth through replacement. However, cartilage can be removed without deformity. - The functional matrix theory viewed skeletal growth as a response to functional soft tissues and spaces



































































