Download to read offline






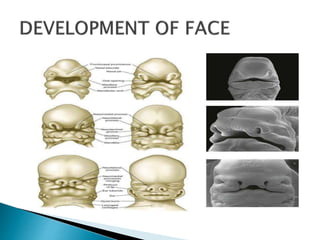
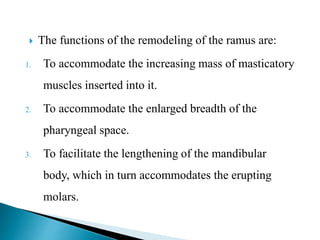
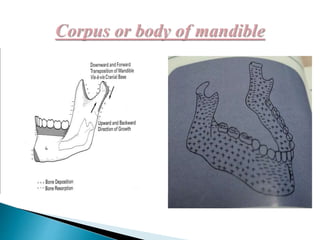
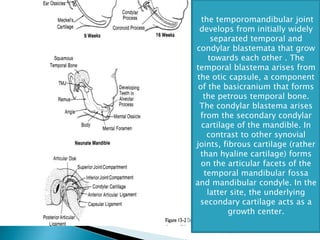






The document discusses the definitions and theories of growth and development, particularly focused on the evolution of the human jaw and craniofacial region from prenatal through postnatal stages. It highlights key growth patterns, structural developments, and the complexities of growth mechanisms influenced by various factors. Additionally, it examines the contributions of different theories and the physical changes in the mandible throughout human development.






















































