Downloaded 31 times

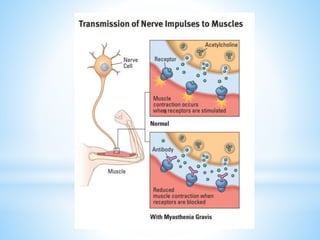
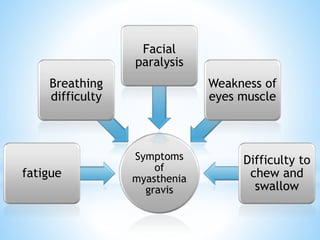
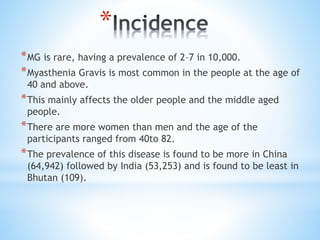

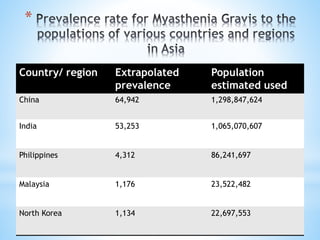


Myasthenia gravis is a rare neuromuscular disorder characterized by muscle weakness that worsens with activity and improves with rest, often affecting eye and facial muscles. It is caused by autoantibodies against neuromuscular junction proteins, with treatment options including immunosuppressive drugs and therapies like plasmapheresis and intravenous immunoglobulin. The disorder is most prevalent in older adults, particularly women, with varying prevalence across regions, and can be diagnosed through tests such as the edrophonium test and electromyography.
























![Myelin Oligodendrocyte Glycoprotein (MOG) Antibody Disease [MOG-AD]](https://cdn.slidesharecdn.com/ss_thumbnails/myelinoligodendrocyteglycoproteinmogantibodydisease0920-200920055159-thumbnail.jpg?width=640&height=640&fit=bounds)

























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




