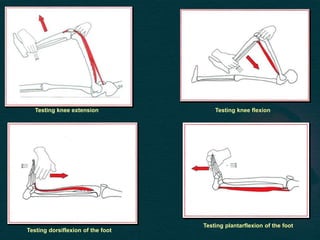
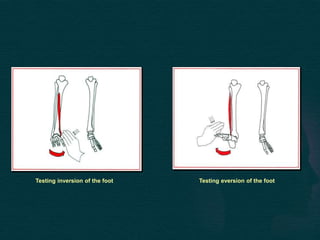
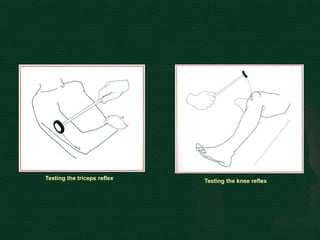
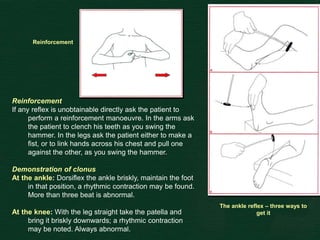
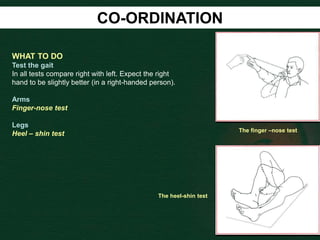
This document provides guidance on performing a motor and sensory examination. It describes how to assess the motor system by examining tone, muscle strength, and reflexes in the arms and legs. It also provides details on evaluating five sensory modalities - vibration, joint position, light touch, temperature, and two-point discrimination. Coordination is assessed using finger-nose and heel-shin tests. Finally, the document outlines how to observe a patient's gait and what various abnormalities may indicate. The overall screening neurological exam is summarized in 3 sentences or less.





























































![Invasive_Cardio-Devices_procedures[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/invasivecardio-devicesprocedures1-240129085722-eb86cfb0-thumbnail.jpg?width=640&height=640&fit=bounds)
































