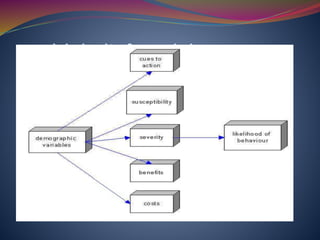
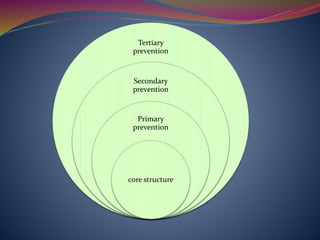
The document discusses various definitions and models of health, prevention, and nursing's role in health promotion. It defines health according to WHO and describes views that health is more than just the absence of disease. It also summarizes levels of prevention from primordial to tertiary. Several health models are explained briefly, including Health Belief Model, Health Promotion Model, Neuman Systems Model, and Nightingale's Environmental Theory. Health promotion frameworks like PRECEDE-PROCEED and OMAHA System are also summarized. Milio's framework for prevention focusing on community-oriented care is described.






















































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)

![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)