Downloaded 45 times
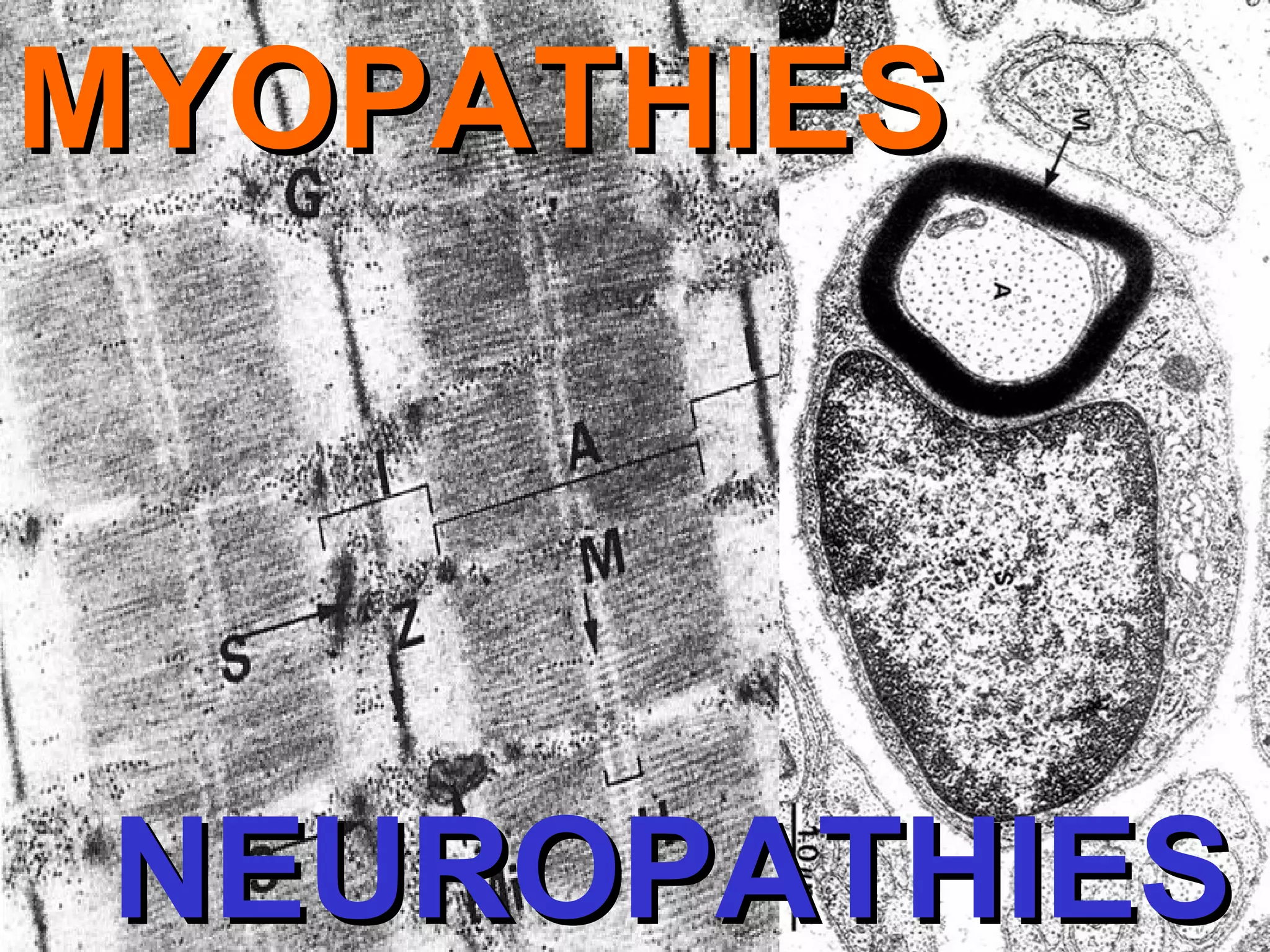
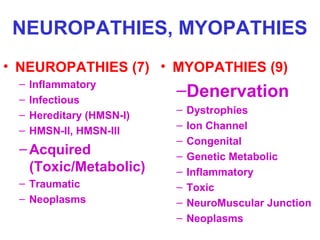
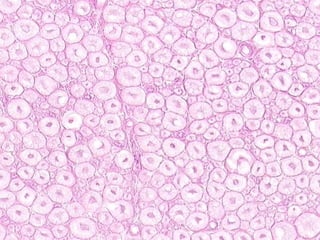
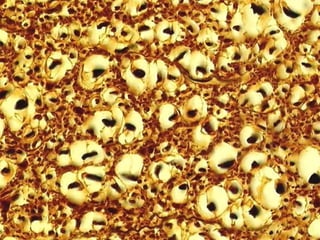
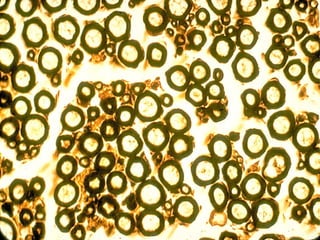
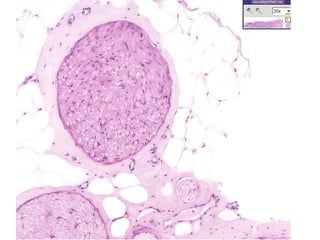
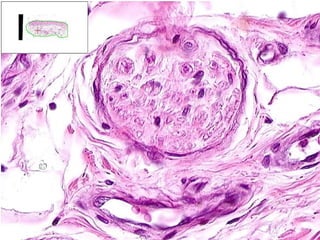
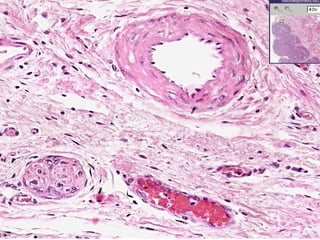
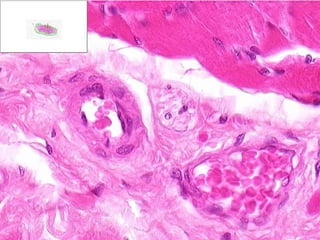
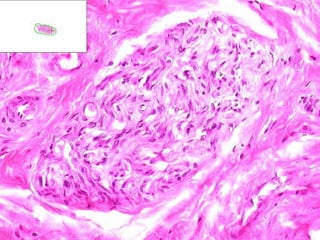
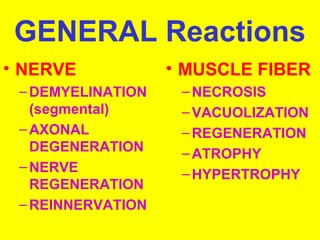
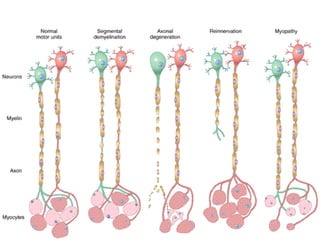

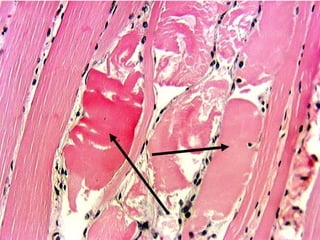
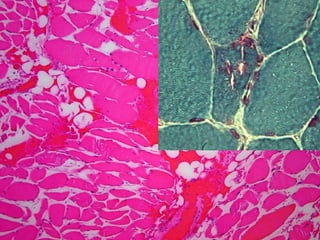
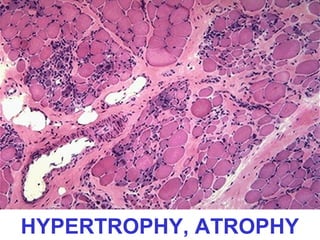

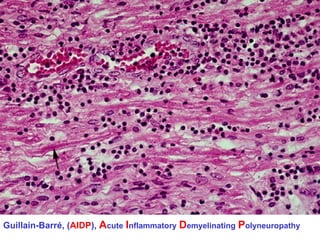

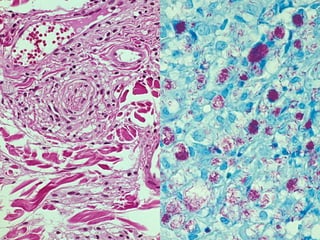
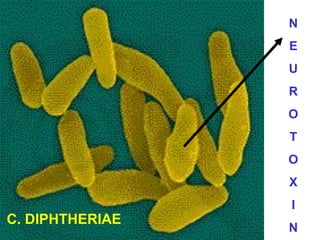



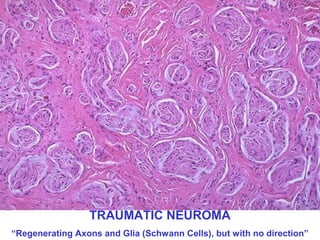
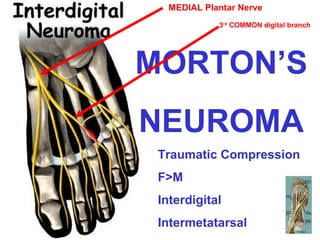


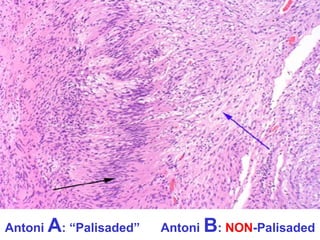
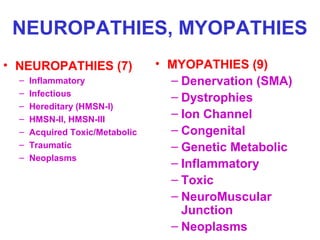
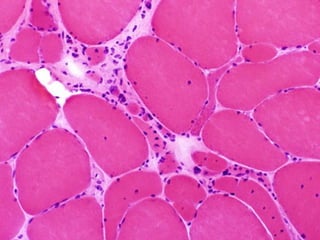
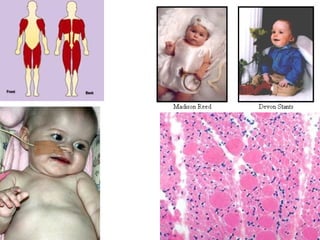
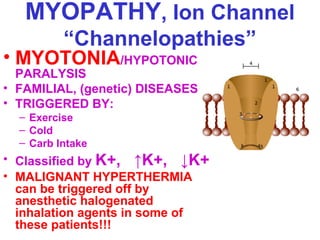
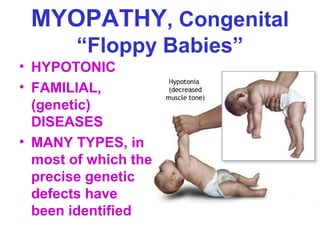
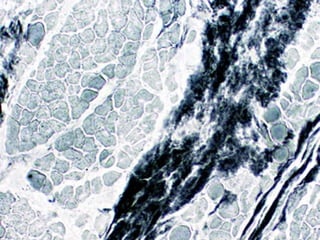
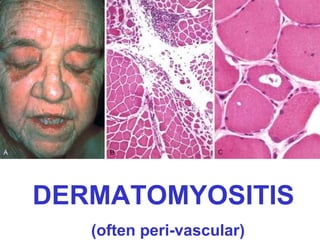
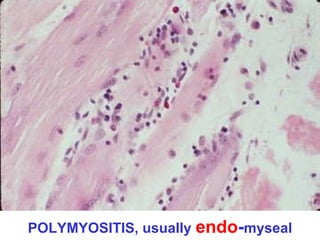
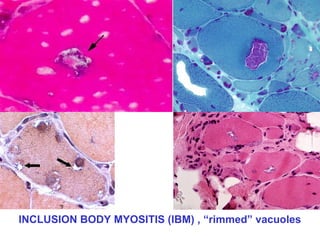


This document discusses neuropathies and myopathies. It lists various types of neuropathies including inflammatory (such as Guillain-Barré syndrome), infectious (such as leprosy), hereditary (such as Charcot-Marie-Tooth disease), toxic/metabolic, traumatic, and neoplastic. It also lists various types of myopathies including denervation, dystrophies, ion channel, congenital, genetic/metabolic, inflammatory, toxic, neuro-muscular junction, and neoplastic disorders. For both neuropathies and myopathies it provides brief descriptions and examples of conditions within each category.



















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



