Downloaded 11 times

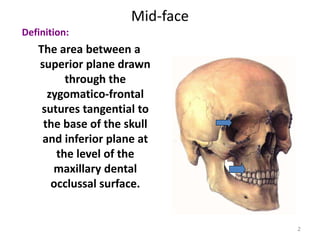
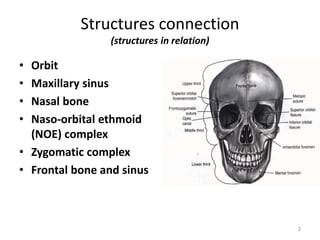
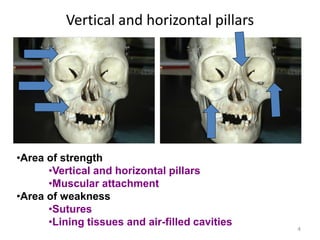


The document outlines the definition of the mid-face, its structure relations, and the aims of treatment for injuries in this area. It discusses factors affecting the risk of complications and principles for treatment, highlighting when closed or open reduction is appropriate. Additionally, it details various fixation and immobilization techniques used in treatment.























































































