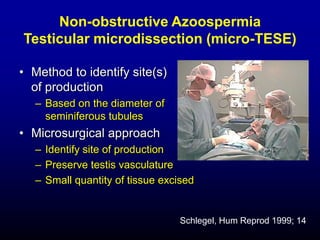
Downloaded 178 times







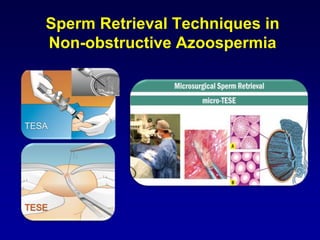
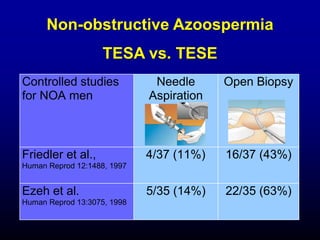






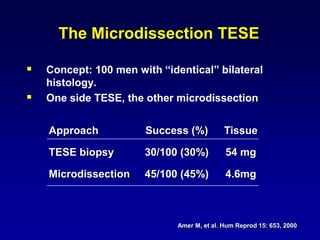
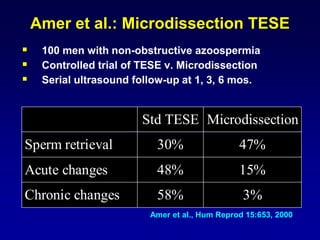

















This document provides an overview of sperm retrieval techniques for non-obstructive azoospermia (NOA). It discusses that sperm retrieval rates are related to testicular histopathology, not etiology of azoospermia. Microdissection TESE has higher sperm retrieval rates than standard TESE, especially for men with maturation arrest or Sertoli cell only syndrome. The chances of sperm retrieval and live birth through ICSI are dependent on the type of azoospermia, with higher success rates for obstructive versus non-obstructive causes.











































































































