Downloaded 90 times

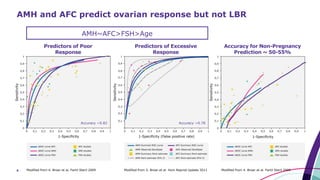

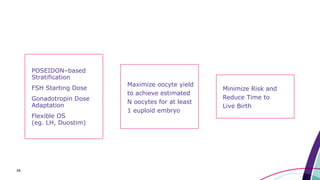
![25 Esteves, Yarali, Ubaldi et al. ESHRE 2019; submitted
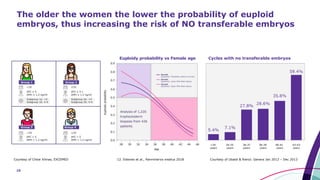
No detrimental effects on embryo ploidy in patients
who retrieve more oocytes
Response Number Euploid Blastocysts
Distribution Binomial
Estimation Method Logistic Regression
Validation Method Validation Column
Probability Model Link Logit
Generalized Regression for number
Euploid Blastocysts Model Launch
Lasso [x] Adaptive
Term Estimate Std Error
Wald
ChiSquare
Prob >
ChiSquare
Lower
95%
Upper
95%
Intercept 6.2769104 0.6256681 100.64771 <0.0001* 5.0506235 7.5031972
Age Female -0.182507 0.152275 143.64894 <0.0001* -0.212352 -0.152662
Number
Blastocysts
0.0302516 0.0189943 2.536584 0.1112 -0.006977 0.0674797
Parameter Estimates for Original Predictors
3,108 Trophectoderm Biopsies
1,109 patients
Euploidy probability vs. number
of blastocysts by age group](https://image.slidesharecdn.com/esteves02mar19isar1100-1200autosaved-190413145746/85/Optimize-oocyte-yield-to-maximize-live-birth-in-ART-25-320.jpg)
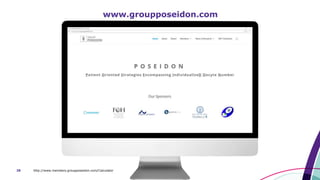
![26
Higher ovarian response than that achieved with mild/natural
ovarian stimulation does not increase risk of embryo aneuploidy
Term Estimate Std Error
Wald
ChiSquare
Prob >
ChiSquare
Lower
95%
Upper
95%
Intercept 3.8117137 1.5331832 6.1809102 0.0129* 0.8067298 6.8166876
Age Female -0.22129 0.019748 125.56789 <0.001* -0.259996 -0.182585
typeOSGrou
ped[Convent
ional-Other]
0.065727 0.33909 0.0375714 0.8463 -0.598877 0.7303311
Response Number Euploid Blastocysts
Distribution Binomial
Estimation Method Adaptive Lasso
Validation Method Validation Column
Probability Model Link Logit
Adaptive Lasso with Validation Column Model Summary
Parameter Estimates for Original Predictors
1,632 Trophectoderm Biopsies by NGS
631 patients
Euploidy probability vs Female Age, by OS Type
Esteves, Yarali, Ubaldi et al. ESHRE 2019; submitted](https://image.slidesharecdn.com/esteves02mar19isar1100-1200autosaved-190413145746/85/Optimize-oocyte-yield-to-maximize-live-birth-in-ART-26-320.jpg)
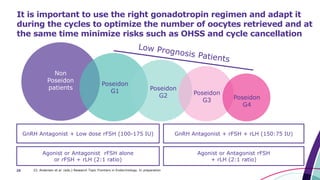
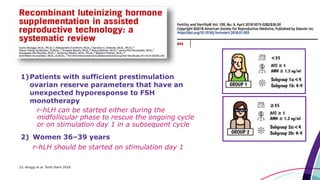
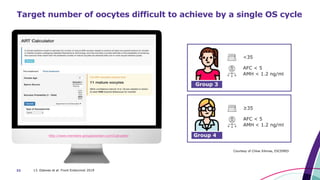
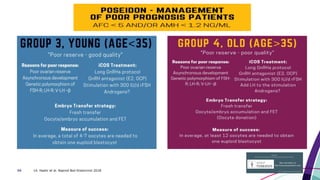
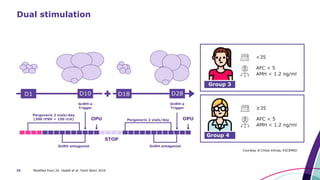


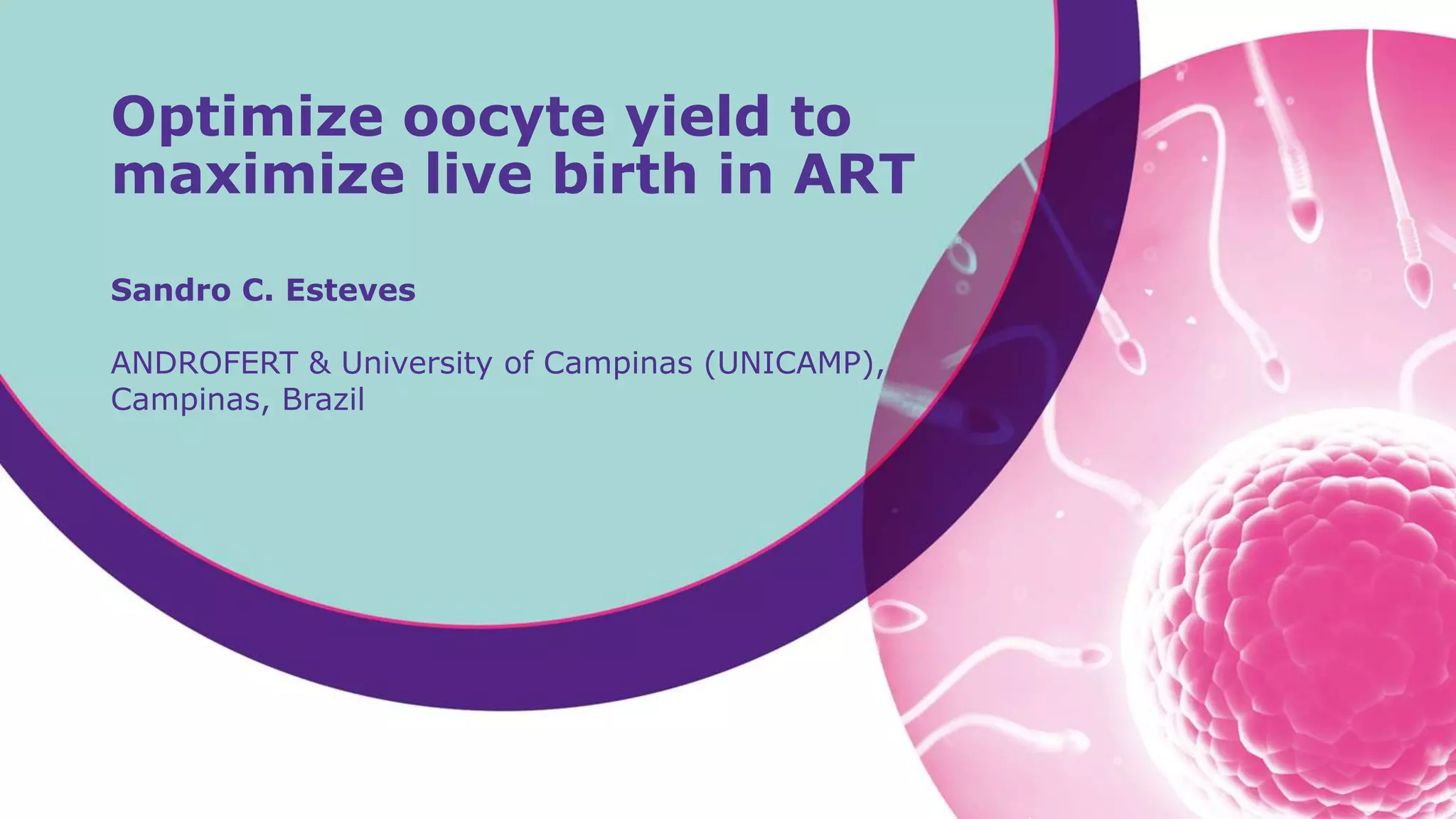
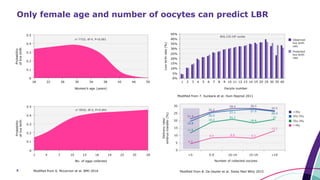
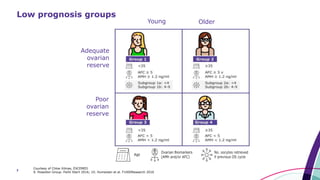
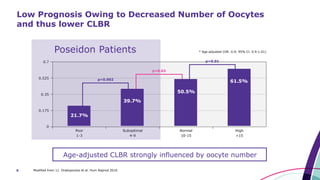
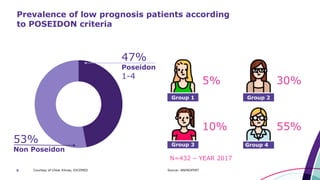
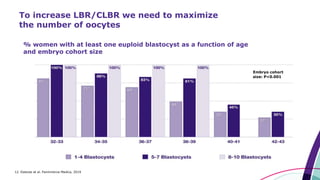
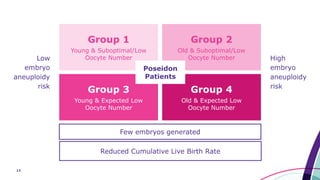
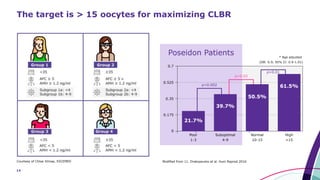
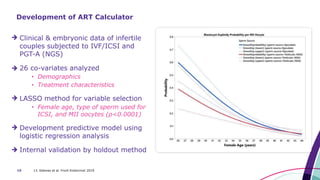
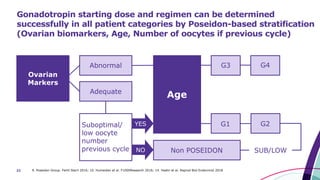
This document discusses strategies for optimizing ovarian response in ART to maximize live birth rates. It introduces the POSEIDON criteria for stratifying "low prognosis" ART patients based on age, ovarian reserve markers, and number of oocytes retrieved. The target is to retrieve over 15 oocytes to maximize cumulative live birth rates. Personalized gonadotropin protocols and adjuvant therapies can be used to optimize response based on POSEIDON stratification. This includes starting dose, supplementation with LH, and dual stimulation if needed to obtain the estimated number of oocytes for at least one euploid embryo transfer.























































































