Downloaded 43 times



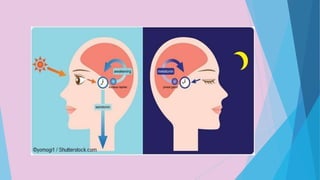







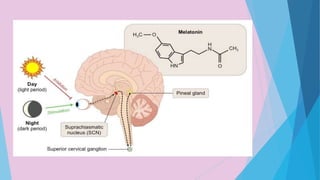

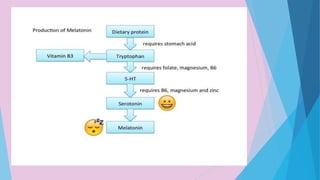



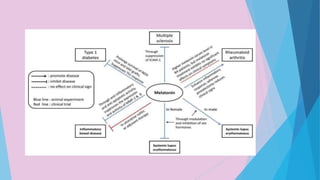











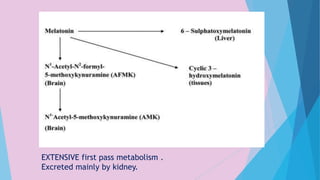

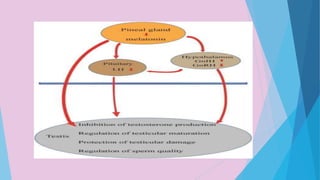




















This document discusses melatonin, including its sources, receptors, biosynthesis, physiological roles, therapeutic uses, and causes of low levels. Melatonin is a hormone secreted in darkness that affects circadian rhythms and is found in many living things. It has roles in sleep, diabetes, and inflammatory conditions. Melatonin levels can be low due to factors like alcohol, caffeine, medications, and stress. Several melatonin supplements and medications are discussed for uses like insomnia, depression, and circadian rhythm disorders. Adverse effects are outlined for different doses.