Download to read offline












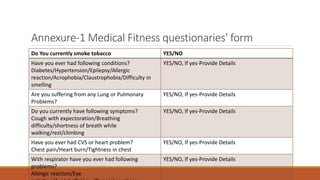





This document outlines a standard operating procedure for a respiratory protection plan. It describes the purpose of conducting medical evaluations to determine an employee's ability to use a respirator. The objectives are to prevent occupational illness and injuries. The SOP applies to employees required to wear respirators during work and emergencies. Components include environmental monitoring, engineering controls, respirator selection, training, and medical examinations. Duties of the program administrator include hazard assessment, respirator selection, training, and record keeping.