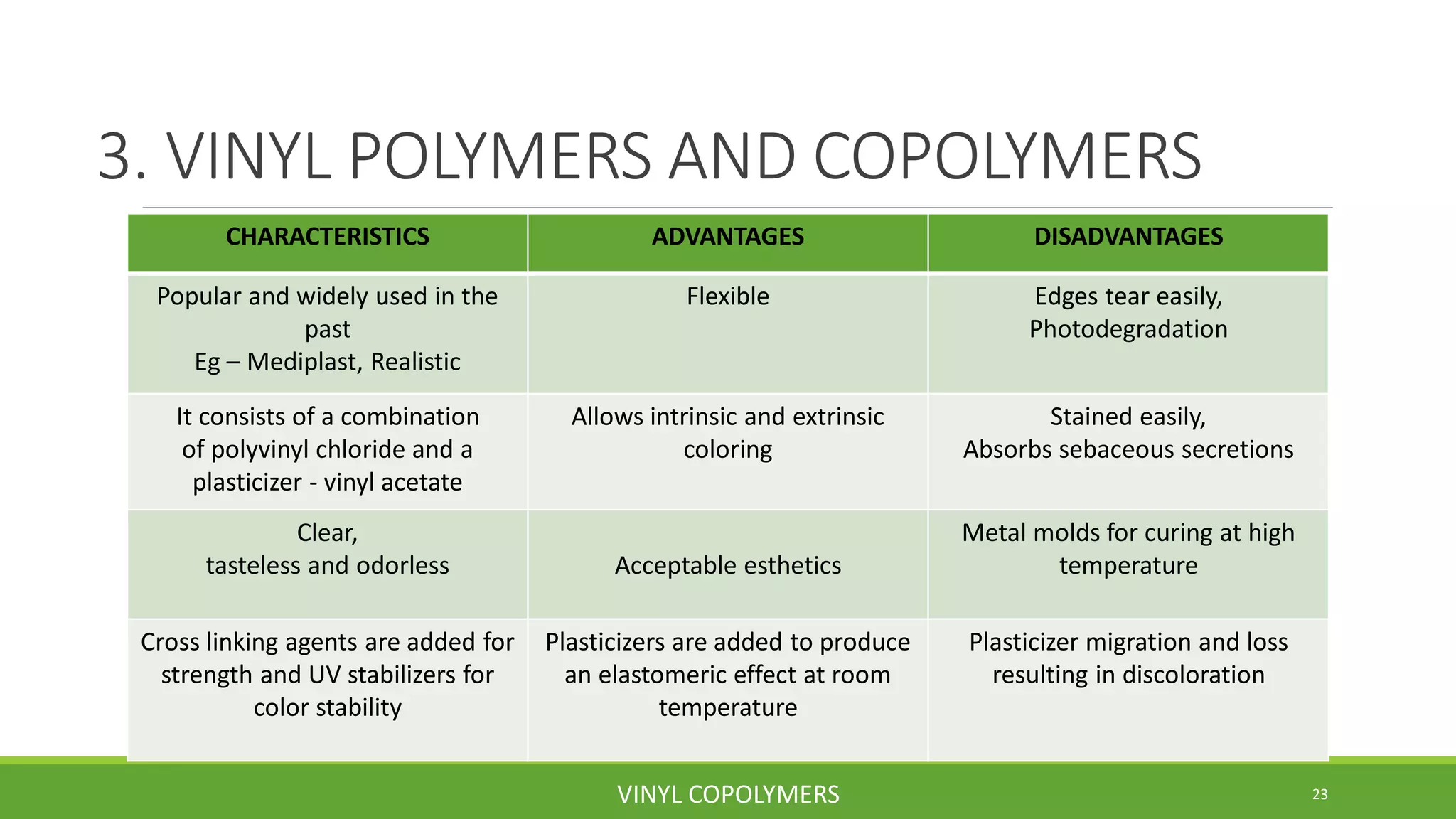
This document discusses maxillofacial materials and prosthetics. It begins with definitions of maxillofacial prosthetics and then discusses the history and characteristics of materials. The key materials discussed include acrylic resins, acrylic resin copolymers, vinyl polymers/copolymers, polyurethane elastomers, and silicone elastomers. The document provides details on the composition, advantages, and disadvantages of each material class. It also discusses classification of materials, coloration, retention, limitations, and recent advances in maxillofacial prosthetics materials.