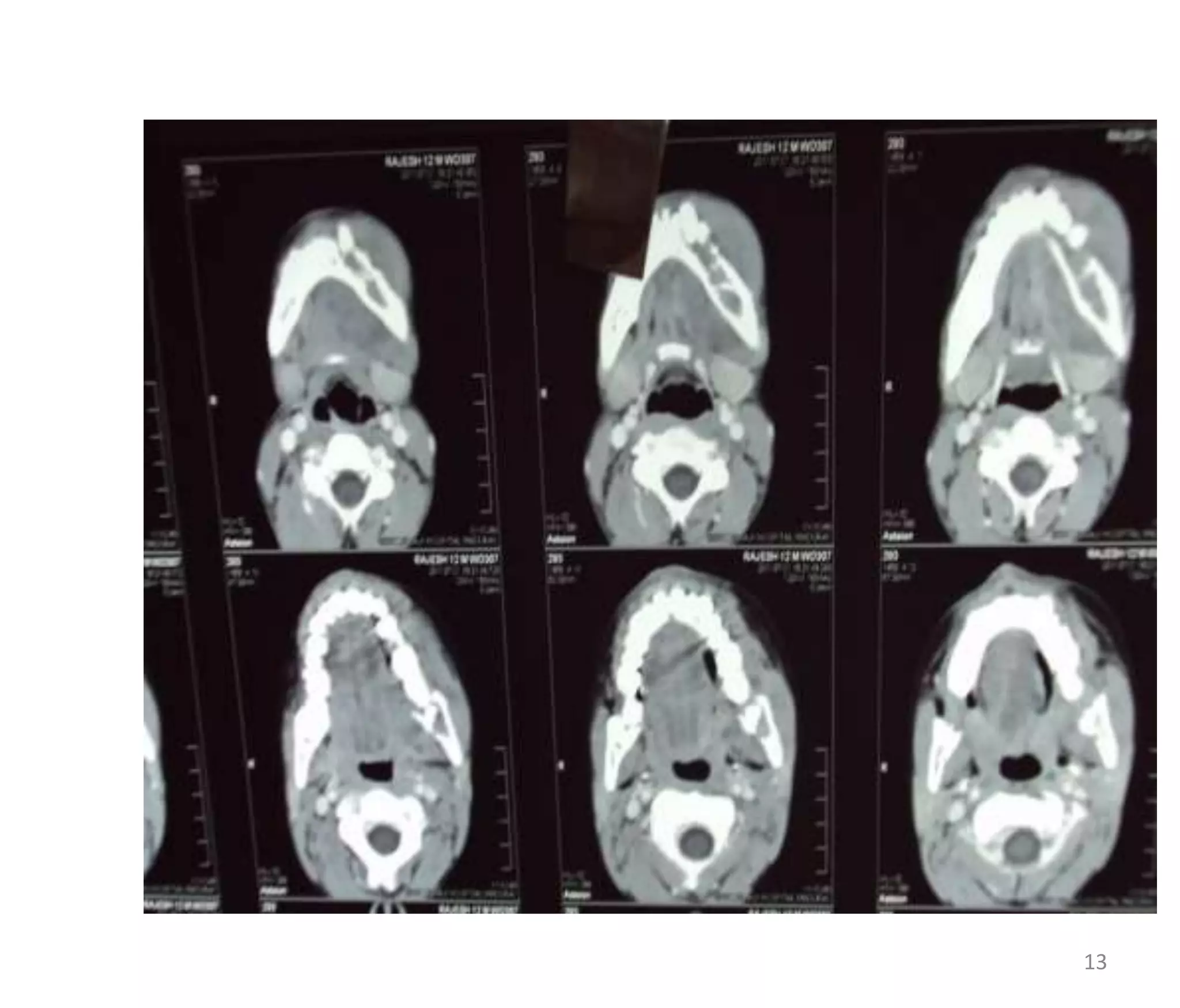
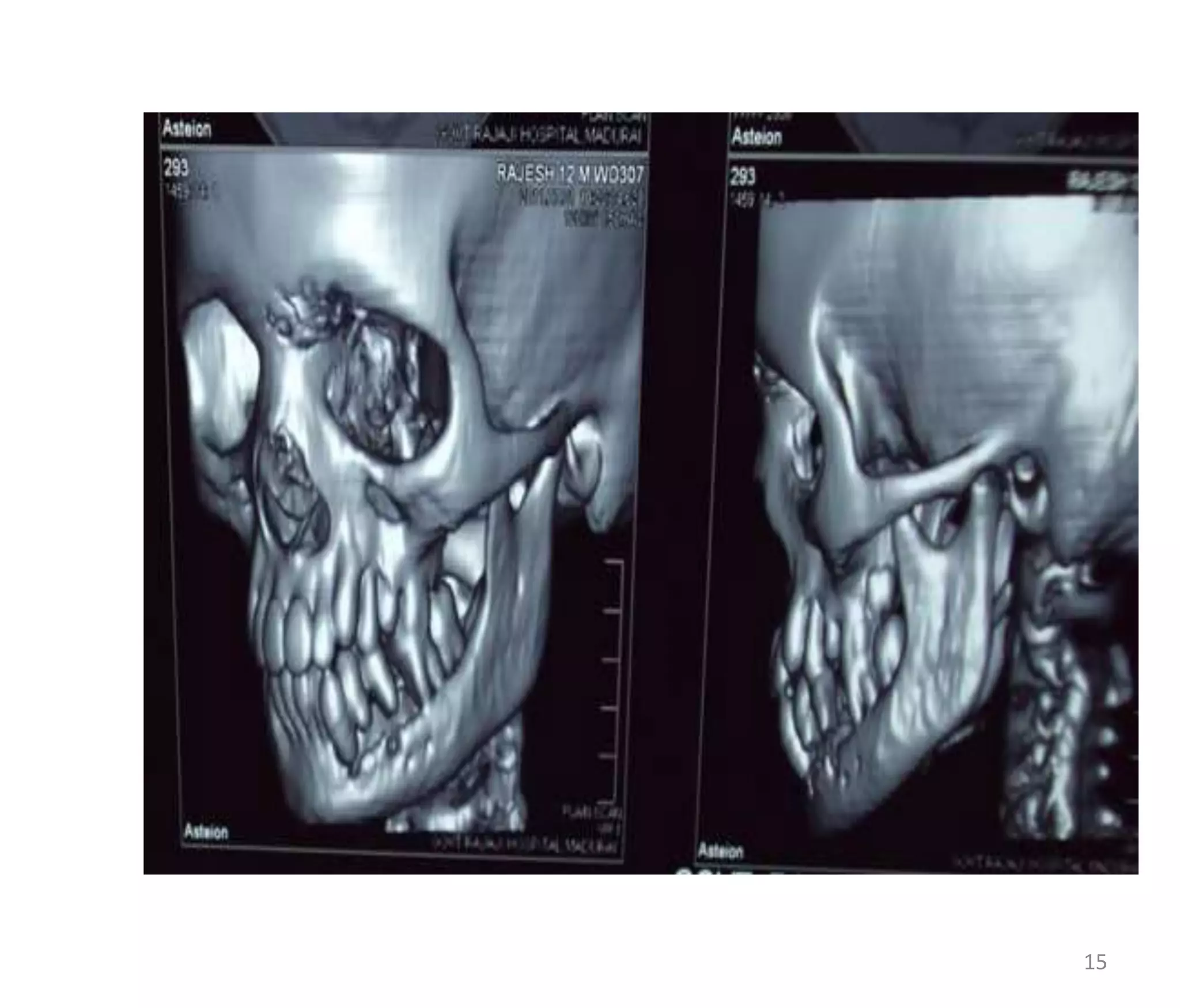
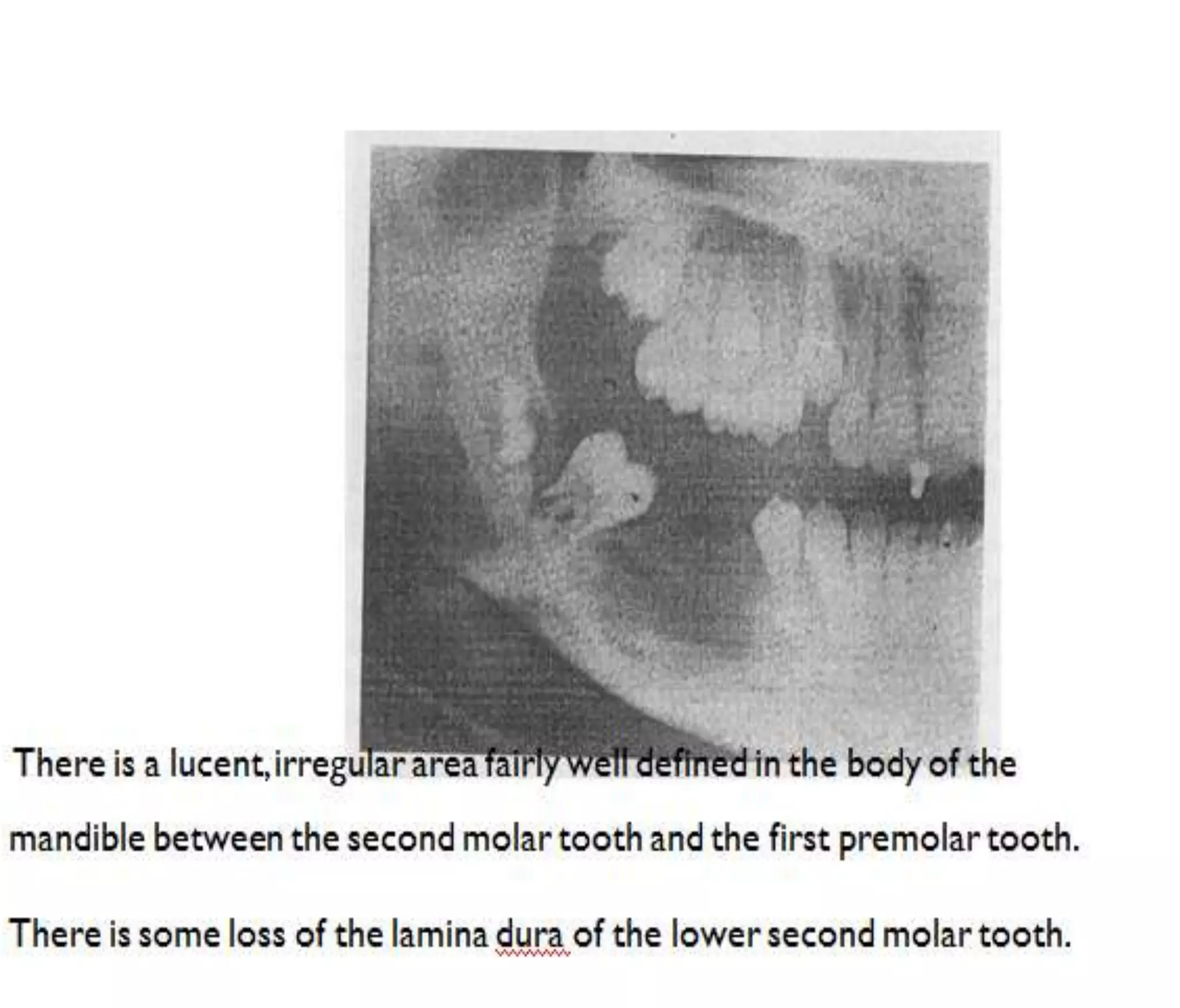
This document presents a case study of a 12-year-old male patient with a swelling on the left side of his jaw that had been present for one month. Examination revealed a 5x4 cm swelling involving the left mandible with tooth resorption and cervical lymph nodes present. X-rays showed an ill-defined lytic lesion in the left mandible with destruction of the alveolar margin and teeth. CT scans further characterized a soft tissue mass extending from the mandible. Differential diagnoses discussed included ameloblastoma, central giant cell granuloma, eosinophilic granuloma, lymphoma, and Ewing's sarcoma based on the patient's presentation and imaging findings.