Download to read offline





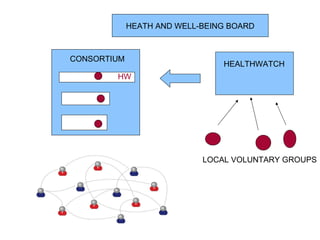





PPI (patient and public involvement) is imperative for successful commissioning for several reasons: it saves money and ensures pathways are used; it increases the moral and democratic legitimacy of the NHS; and it leads to safer and better designed services. Effective PPI requires democratic and participatory involvement from both individuals and community groups to influence priorities, service development, and quality standards. This can be achieved through structures like Healthwatch, consortium governance models, and community development approaches that view community members as assets and work to improve health through co-production.




































































![York integration seminar [5.4.12] (c brand et al)](https://cdn.slidesharecdn.com/ss_thumbnails/yorkintegrationseminar5-4-12cbrandetal-121014152821-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



























