Downloaded 12 times



![SOCIAL NETWORKS
REDUCE MORTALITY RISK
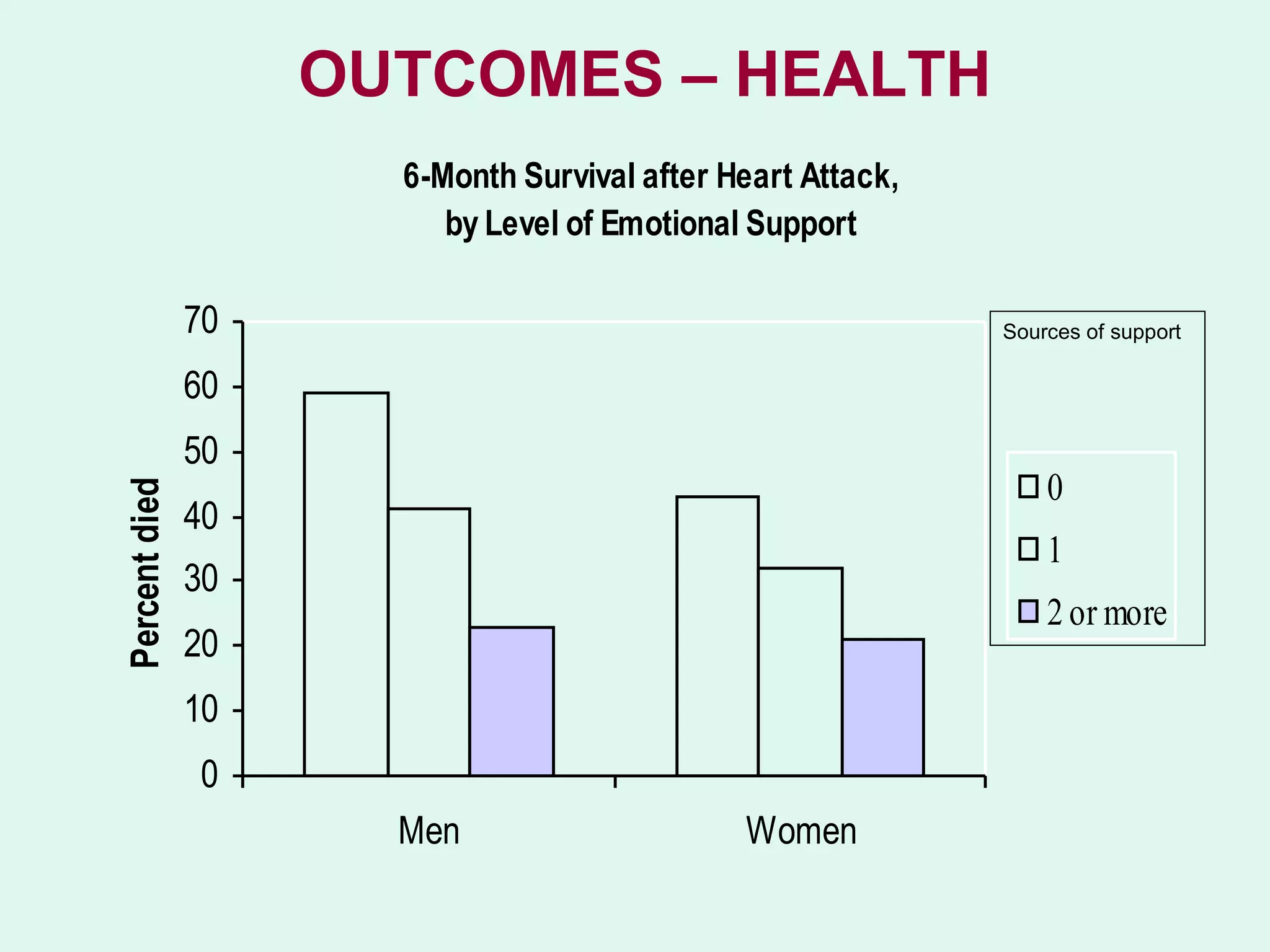
• 50 % increased likelihood of survival for people with
stronger social relationships
• Comparable with risks such as smoking, alcohol, BMI
and physical activity.
• Consistent across age,
sex, cause of death.
• 2010 meta-analysis of data [1] across 308,849 individuals,
followed for an average of 7.5 years
1] Social relationships and mortality risk: a meta-analytic review. Holt-Lunstadt, Smith, Bradley
Layton.Plos Medicine July 2010, Vol 7, Issue 7. www.plosmedicine.org
doi:10.1371/journal.pmed.1000316](https://image.slidesharecdn.com/kendallcdtoynbee-1-130208042551-phpapp02/75/Community-Development-and-Health-10-2048.jpg)
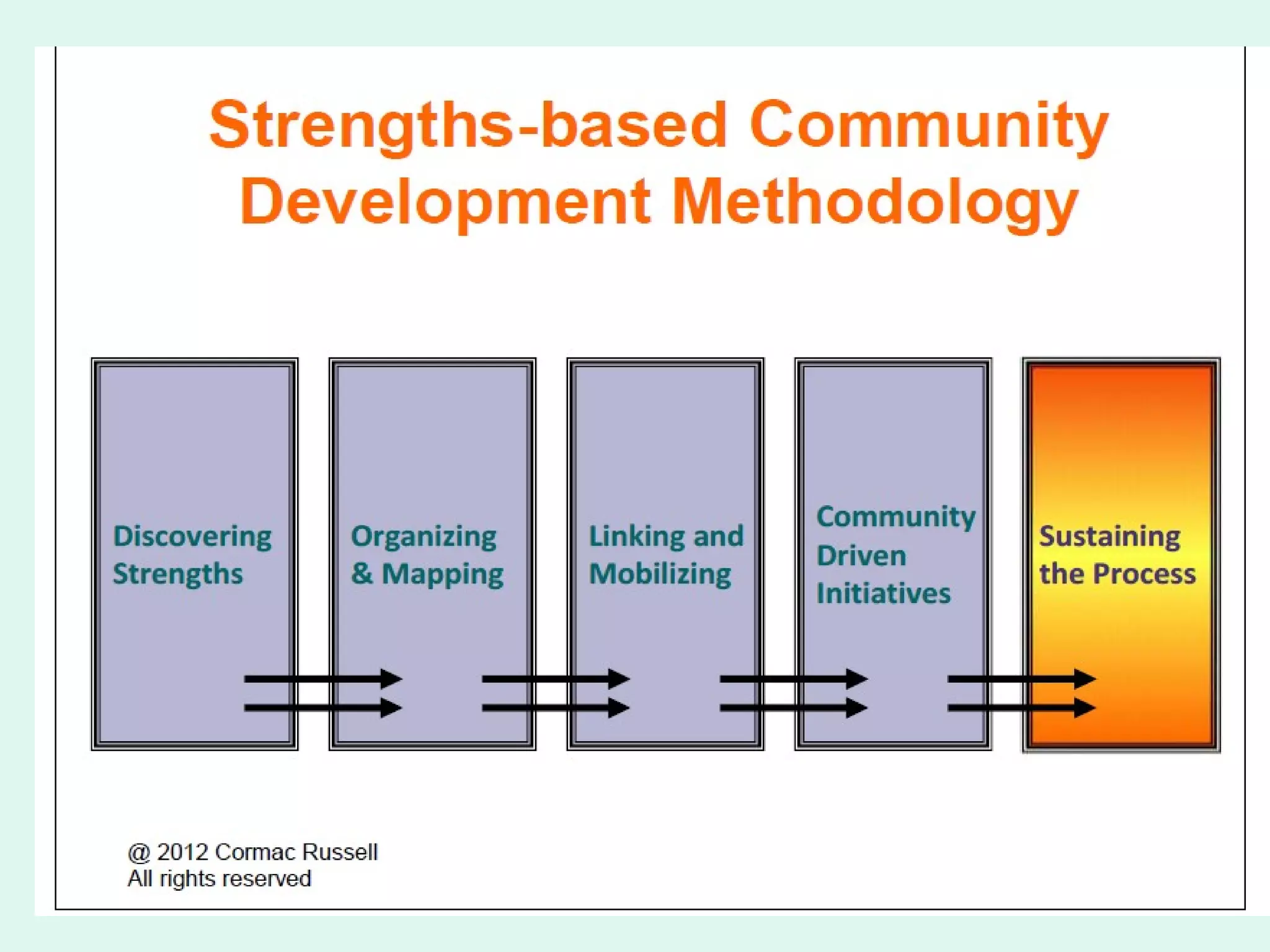






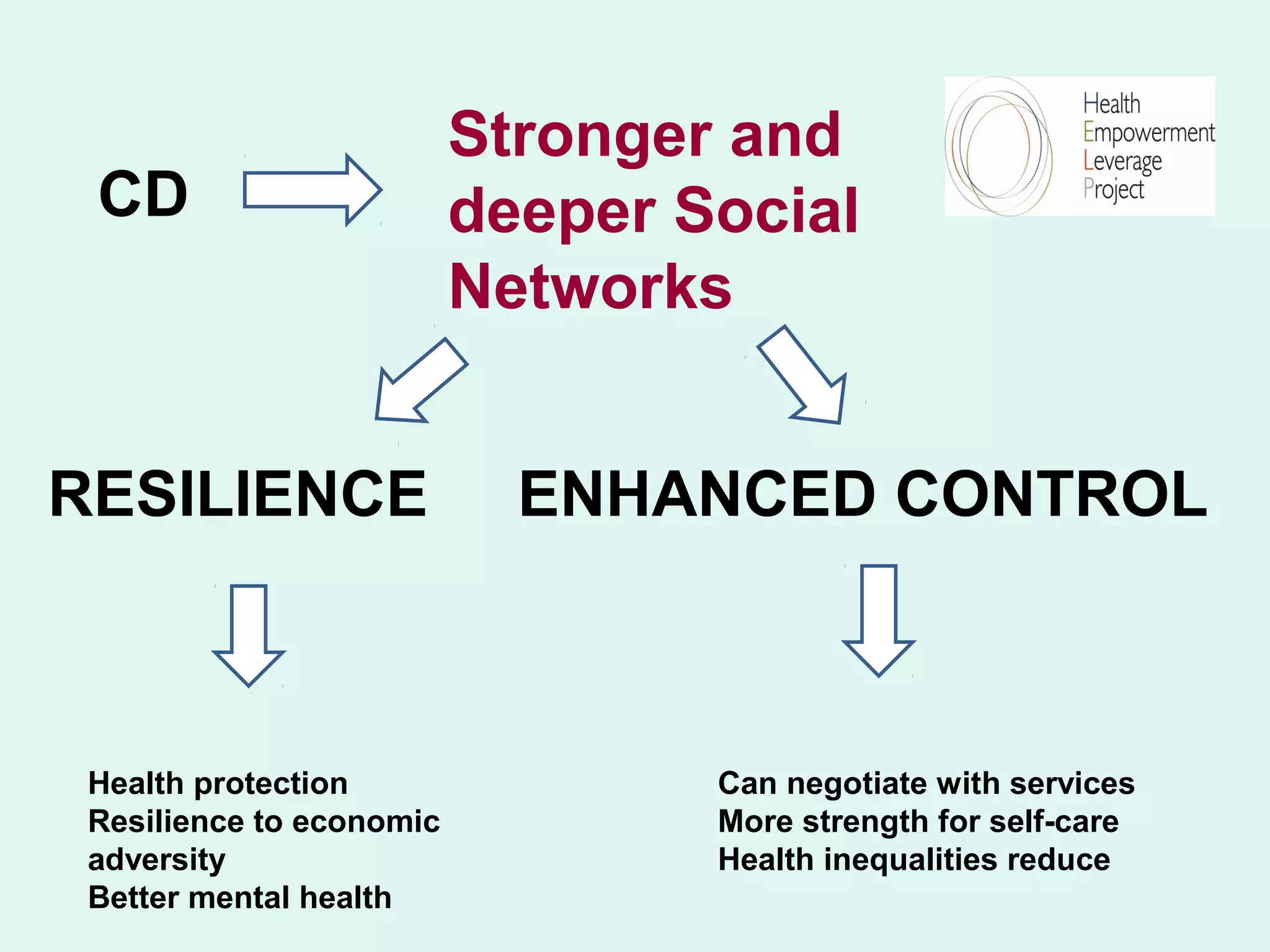
This document discusses the negative impacts of austerity and shrinking the state, including threats to mental health, weakened social networks, and democratic accountability. It advocates for asset-based community development and participatory accountability to promote community resilience, tackle health inequalities, and save money. Strong social networks are shown to reduce mortality risk and enhance control. A resident-led partnership approach can lead to responsive services that address community needs and improve outcomes. Modest investments in these programs can yield high social returns through health and social benefits.


























































![York integration seminar [5.4.12] (c brand et al)](https://cdn.slidesharecdn.com/ss_thumbnails/yorkintegrationseminar5-4-12cbrandetal-121014152821-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



























