Download to read offline

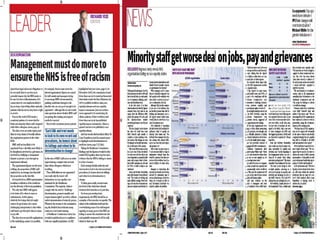



The document discusses race equality past, present, and future in the NHS. It summarizes that institutional racism can be detected through unwitting prejudice, ignorance and thoughtlessness that disadvantages ethnic minority people. Current legislation aims to eliminate unlawful discrimination and promote equality. However, evidence shows ethnic minority NHS staff are underrepresented in senior roles and overrepresented in disciplinary actions. Data on ethnic minority patient experiences is also lacking. The NHS BME Network vision is to ensure the NHS delivers on race equality duties through an independent voice for ethnic minority staff, patients, and service users. Changes are needed like eliminating workplace discrimination and ensuring quality care for all.















































![York integration seminar [5.4.12] (c brand et al)](https://cdn.slidesharecdn.com/ss_thumbnails/yorkintegrationseminar5-4-12cbrandetal-121014152821-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




















