Downloaded 11 times


![SOCIAL NETWORKS
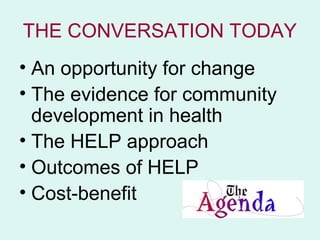
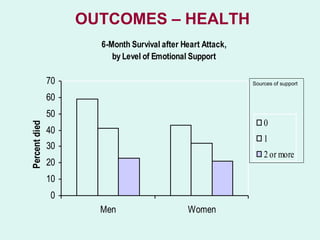
REDUCE MORTALITY RISK
• 50 % increased likelihood of survival for people
with stronger social relationships .
• Comparable with risks such as smoking, alcohol,
BMI and physical activity.
• Consistent across age,
sex, cause of death.
• 2010 meta-analysis of data [1] across 308,849 individuals,
followed for an average of 7.5 years
1] Social relationships and mortality risk: a meta-analytic review. Holt-Lunstadt,
Smith, Bradley Layton.Plos Medicine July 2010, Vol 7, Issue 7.
www.plosmedicine.org doi:10.1371/journal.pmed.1000316](https://image.slidesharecdn.com/communitydevelopmenttransformationanddeprivedcommunities-120918025351-phpapp01/85/Community-development-transformation-and-deprived-communities-9-320.jpg)





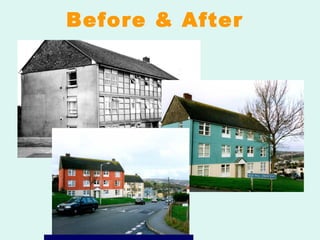
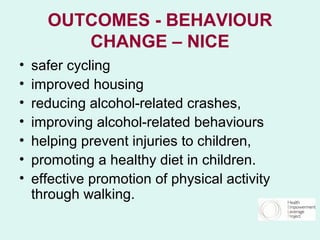
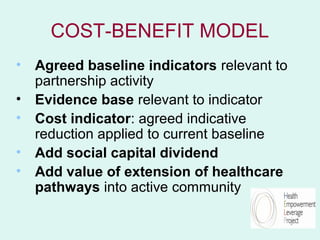
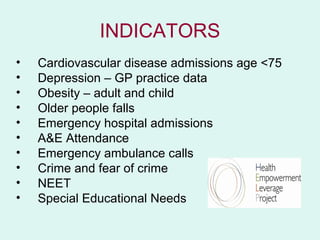

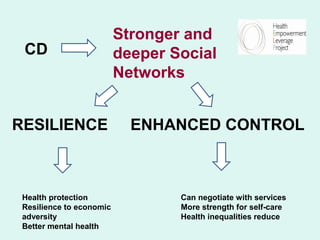
This document discusses community development and its potential benefits for improving population health outcomes. It summarizes the HELP (Health Empowerment Leveraging Partnerships) project approach, which involves working with local residents and services to tackle issues, build social networks and make services more responsive. Evidence suggests that stronger social networks can reduce mortality risk and help address health inequalities. The HELP model has led to improved outcomes such as more responsive local services and reductions in health indicators like CVD admissions. Cost-benefit analysis indicates the HELP approach can save money compared to the investment required.


























































![York integration seminar [5.4.12] (c brand et al)](https://cdn.slidesharecdn.com/ss_thumbnails/yorkintegrationseminar5-4-12cbrandetal-121014152821-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







