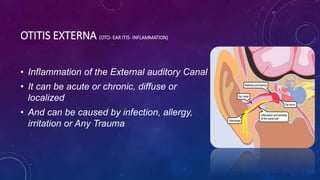
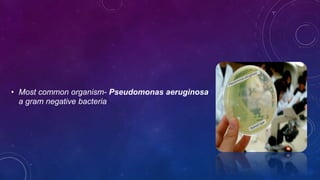
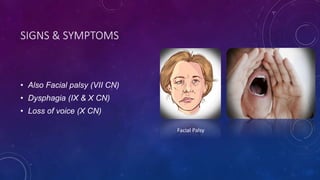
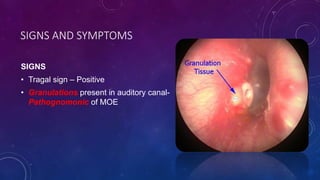
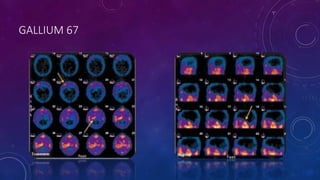
Malignant otitis externa is a severe inflammatory condition of the outer ear canal, often caused by infections such as Pseudomonas aeruginosa, primarily affecting elderly and immunocompromised individuals. Symptoms include intense ear pain, purulent discharge, and potential facial nerve involvement, and diagnosis is aided by imaging techniques like CT scans and gallium-67 scans. Treatment involves long-term antibiotics and managing underlying conditions, emphasizing the importance of early diagnosis and regular follow-ups.