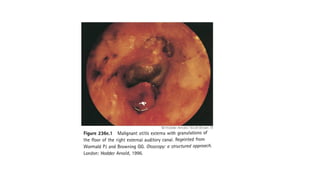
MALIGNANT OTITIS EXTERNA
•DEFINITION :
Malignant otitis externa is an aggressive and potentially life-
threatening infection of the soft tissues of the external ear and
surrounding structures, quickly spreading to involve the periosteum
and bone of the skull base.
5.
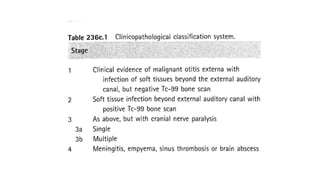
• STAGING :
•Three different staging systems for malignant otitis externa have been
suggested.
• All have a three stage system and they combine clinical and
radiological features.
• Each has its advantages, but none is comprehensive. By combining
the existing staging methods, a modified, more adequate
clinicopathological classification system can be achieved.
7.
• PATHOLOGY:
• Malignantotitis externa is the end -stage of a severe infection that
originates from the external auditory canal and progresses through
cellulitis, chondritis, periostitis, osteitis and finally osteomyelitis.
• Infection is thought to spread out of the cartilaginous external
auditory canal through the fissures of Santorini, congenital defects in
the floor of the external auditory canal.
8.
• Once periostitisdevelops, this progresses rapidly across the skull
base. As a result, facial nerve and other cranial nerve palsies are
sustained. Once the periostitis is well developed, osteomyelitis ensues
as a secondary phenomenon.
• Malignant otitis externa mainly affects the Haversian system of
compact bone and involvement of the pneumatized portion of the
temporal bone is a late finding. The otic capsule is usually spared.
Multiple microabscesses are found at surgery or post-mortem.
9.
• Bacteriology :
Pseudomonasaeruginosa is the most common pathogen (95% of cases).
Rarely, aspergillus can cause malignant otitis externa.
• Predisposing factors:
It most commonly affects elderly diabetic (both type I and type II) patients who
may have an impaired host response to Pseudomonas via several different
immunological mechanisms, including impaired leukocyte mobility.
However, the microangiopathy in diabetic tissues, exacerbated by the vasculitic
properties of Pseudomonas has been postulated to be more important.
Impairment of phagocytosis is usually due to 'hyperglycexternal auditory
canalia' which is more common in younger type I diabetics. In many cases of
malignant otitis externa, only a mild impairment in glucose tolerance is seen.
10.
• The cerumenin diabetic patients is also of a higher pH than that of
normal controls, which may reduce the bactericidal properties of
their cerumen.
• Children more commonly have a facial nerve palsy and involvement of
the middle ear. Refractory or suspected malignant otitis externa in
children or adults can be caused by histiocytosis or malignancy of the
temporal bone and this often needs to be excluded by biopsy of
granulations.
• Other causes of immunocompromise, especially conditions that affect
cell-mediated immunity (e.g. AIDS), can also predispose to malignant
otitis externa, although it is postulated that infection in these
individuals starts in the middle ear and is frequently caused by
organisms other than Pseudomonas.
11.
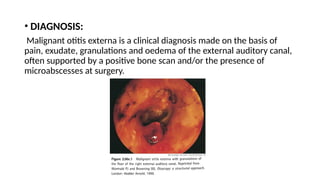
• DIAGNOSIS:
Malignant otitisexterna is a clinical diagnosis made on the basis of
pain, exudate, granulations and oedema of the external auditory canal,
often supported by a positive bone scan and/or the presence of
microabscesses at surgery.
12.
• Diabetes orother immunocompromised state, Pseudomonas
aeruginosa on culture, a positive bone scan and cranial nerve palsy
are confirmatory factors that enhance the specificity of the diagnosis.
• ESR and CRP levels are nonspecific measures of inflammation that are
significantly raised in untreated cases and are useful barometers with
which to measure response to treatment. The ESR is often over 100
mm/hour.
13.
• RADIOLOGY:
• Technetium(Tc-99m) radio nuclide bone scans will detect bony involvement
even before high-resolution computed tomography (CT) scans can
demonstrate bone destruction. As the isotope is absorbed by osteoclasts and
osteoblasts that continue remodelling after the infection has resolved, the
scan may remain positive for up to nine months. As such, Tc-99m is only
useful for detecting initial bony involvement.
• Gallium (Ga-67) is absorbed by leukocytes and is a more sensitive monitor of
infection. The scan quickly returns to normal after the infection has resolved
and as such, is a good measure to ascertain when to terminate treatment.
• Ga-67 is taken up by any inflammatory process, including simple otitis
externa and it is useful for monitoring rather than diagnosis. By combining
either of these radioisotopes with CT (SPECT), good spatial localization of
disease extent and anatomy can be obtained.
14.
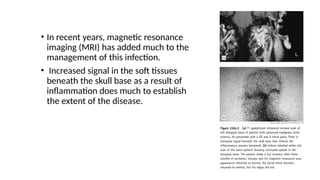
• In recentyears, magnetic resonance
imaging (MRI) has added much to the
management of this infection.
• Increased signal in the soft tissues
beneath the skull base as a result of
inflammation does much to establish
the extent of the disease.
15.
• OUTCOMES ANDCOMPLICATIONS:
• The mortality and complication rate from malignant otitis externa has
dramatically decreased. In Chandler's initial series, there was an overall
mortality of 46 percent but this has dropped to below 10 percent with
aggressive management and early diagnosis.
• The presence of a cranial nerve palsy is a sign of advanced disease and these
patients can still have mortality rates of up to 80 percent. If the disease
progresses, extensive skull base osteomyelitis becomes established.
• The clivus and contralateral temporal bone can be involved and infection can
spread anteriorly into the sphenoid and to the carotid. Anterior infection can
involve the temporomandibular joint and parapharyngeal space.
•
16.
• The facialnerve is the most commonly affected cranial nerve (60
percent of cases with palsies) and thereafter the IX, X and X cranial
nerves. Paralysis of the VI or XII cranial nerves is rare. Finally, disease
can spread to the central venous sinuses, extradural space and
meninges.
• Infective thrombophlebitis or thrombosis of the internal carotid artery
are the usual terminal events. If the disease is sucessfully treated,
facial palsy may completely resolve in 22 percent, with a partial
recovery seen in a further 9 percent.
17.
• MANAGEMENT OPTIONS:
•Aural toilet: Local toilet to the external auditory canal is essential to
control the granulations and improve local pain control.
• The use of topical antibiotics is controversial. They are likely to alter
the microbiological flora of the external auditory canal.
18.
• Systemic antibiotics:
• The treatment of choice for the management of malignant otitis
externa is systemic anti-Pseudomonas antibiotics.
• The drug often needs to be given for at least six weeks and in
advanced cases, several months. These are often given initially, with
transition to oral antibiotics once the CRP and ESR start to fall.
• Fluoroquinolones rapidly achieve high levels in the serum and tissues
when administered orally. Cure rates of over 95 percent have been
reported in a review of 13 publications.
• Oral rifampicin can also be added, although it is unclear whether this
adds anything in terms of improved outcomes. Resistance to
fluoroquinolones appears to be increasing from 10 percent in the
early 1990s to 56 percent (five of nine) more recently.
19.
• Hyperbaric oxygen:
•Hyperbaric oxygen treatment is often used in centres with easy
access to hyperbaric chambers.
• Surgery :
• Surgical intervention for malignant otitis externa should be reserved
for a few selected cases and no longer has the goal of removing all the
infected tissue.
• Surgery for the removal of sequestra, collections of pus and
debridement of necrotized and granulating tissues can be beneficial,
but should only be used if the patient is deteriorating clinically and if
definable surgical goals can be easily achieved.
INTRODUCTION
• Otoacoustic emissions(OAE) are acoustic signals emitted from the cochlea
to the middle ear and into the external ear canal where they are recorded.
• They are most probably generated by active mechanical contraction of the
outer hair cells, spontaneously or in response to sound.
• There are four types of OAEs: spontaneous OAEs (SOAE),
transient evoked OAEs (TOAE),
distortion product OAEs (DPOAE),
stimulus frequency OAEs (SFOAE).
• All four types of OAEs are recorded with a sensitive, low noise microphone
that is placed in the sealed external ear canal.
22.
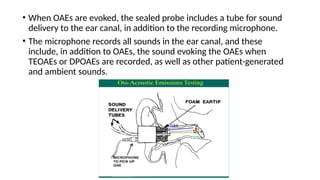
• When OAEsare evoked, the sealed probe includes a tube for sound
delivery to the ear canal, in addition to the recording microphone.
• The microphone records all sounds in the ear canal, and these
include, in addition to OAEs, the sound evoking the OAEs when
TEOAEs or DPOAEs are recorded, as well as other patient-generated
and ambient sounds.
23.
• Because ofthe low level of OAEs and the presence of other sounds in
the ear canal, several measures must be taken to secure reliable
recordings.
• Detection and separation of the low-level OAEs signal from other
sounds recorded in the ear canal require some steps to enhance the
signal and minimize noise.
• Visual inspection, and preferably tympanometric measurement prior
to AOEs recordings, will help determine if middle ear and external ear
abnormalities might reduce or block acoustic transmission of OAEs
from the cochlea to the microphone, and in the case of TEOAEs and
DPOAEs, of the evoking sound to the cochlea.
• Reduction of ambient noise picked up by the microphone is achieved
by a tight fit of the probe into the ear canal.
24.
TRANSIENT-EVOKED EMISSIONS
• Transientevoked otoacoustic emission (TEOAE) is an acoustic
response generated by patient’s cochlea when provided with click or
tone-burst stimulation.
• TEOAE is an indication of auditory receptor’s normal condition. It is
extremely weak acoustic vibrations which can be recorded in external
auditory canal by very sensitive low-noise microphone.
• Emission is widely spread among persons with normal hearing (with
auditory threshold of 25 dB HL or less). In particular, it is a measure of
good hearing at medium frequencies.
25.
• TEOAE techniquecan be used to diagnose various auditory conditions
in the following cases:
• infant hearing screening;
• monitoring of patients with a risk of hearing loss;
• detection of cochlear dysfunction;
• study of cochlear function and getting diagnosis before medical
procedures;
• detection of sensory hearing loss causes.
26.
• TEOAE appearancethresholds of persons with normal hearing are
very close to behavioral hearing thresholds. If patient suffers from
sensory or conductive hearing loss, so that hearing thresholds are 30
dB or worse, emission disappears. That’s the distinctive feature of
TEOAE.
• TEOAE can be successfully recorded at 3-4 days after birth. As TEOAE
sensitivity is very high even to slight hearing impairment, this
technique can be widely used in screening studies of infants.
• TEOAE represents 2-3 (or rarely more) vibration groups of different
frequencies appearing in 6-8 ms after the stimulus beginning and
lasting 20-30 ms.
• After the acquisition you can get the result either in graphic or text
form for further analysis.
27.
• A patientmust be placed in a comfortable and quiet environment,
preferably a sound booth where the patient lies down or sits
comfortably. The patient should relax to reduce noise level.
• To improve acquisition quality, it is recommended to inspect patient's
ear canal. Cleaning of the ear canal shall only be performed by a
person trained in such procedure in order to prevent any irreversible
middle ear damage.
• Pay attention to the OAE probe version and its sensitivity. The
sensitivity (mV/Pa) and the version number are usually indicated on
OAE probe’s label. Before the first use of the program to record OAE,
correct OAE probe version and sensitivity value are set in the program
settings
28.
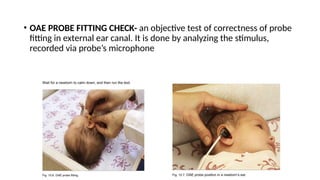
• OAE PROBEFITTING CHECK- an objective test of correctness of probe
fitting in external ear canal. It is done by analyzing the stimulus,
recorded via probe’s microphone
29.
• For goodfitting the OAE probe should comply with the following
requirements:
1. It obturates the external ear canal to convert the small oscillations
of the tympanic membrane to the pressure fluctuations which can
be detected with use of the probe microphone.
2. It prevents contamination of the record with external noise.
3. It provides the required acoustic environment for the generation of
the correct stimuli by the probe telephone.
30.
• To complywith the aforementioned requirements, the OAE probe
should be inserted together with the soft replaceable ear tip.
• The ear tip size is selected after the visual assessment of a patient’s
external ear canal size.
• The delivery set of Neuro-Audio digital system includes cone-shaped
and mushroom-shaped ear tips.
• These ear tips are disposable and should be thrown away after use.
• When the probe is inserted into ear canal, its tip should not be set
against the wall of the external ear canal, because it interferes with
the stimulus presentation and/or OAE acquisition.
33.
Newborn Hearing Screening
•To perform a newborn hearing screening, select “TEOAE (screening)”
test template. The newborn should stay quiet and calm, it is usually
preferred for the infant to be asleep.
• Calm a baby, however, the sucking causes the additional noise and
decreases the probability of test passing.
• Warming the ear tips prior to insertion helps to keep the baby calm.
• The ears of the newborns are often wet or contain the extraneous
masses. If the good stimulation was not obtained at the first insertion
of a probe, replace the ear tip with these extraneous masses by the
new one and try again.
35.
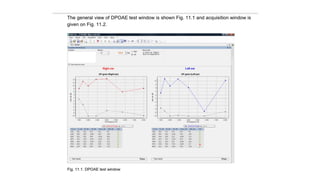
Acquisition and analysis
•Start acquisition with repetitive stimulation using Acquisition|
Repetitive stimulation ([Ctrl+R]) menu command and follow the
process of signal averaging. To cancel the acquisition use Acquisition|
Cancel ([Esc]) menu command.
• To stop the stimulation for some time use Acquisition|Pause [space
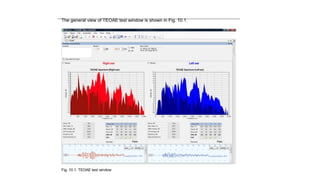
key] menu command. The acquisition window is represented on Fig.
10.8.
37.
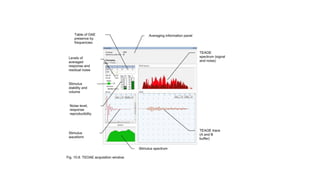
• The toppart of the acquisition window contains the standard
averaging information panel.
• The number of averaged and rejected traces and also the current
stage of TEOAE acquisition are displayed on it.
• The “Averaging” tab displays parameters of the stimulus (recorded via
the OAE probe microphone) and response, including the trace shape
and spectrum.
• Stages of TEOAE Acquisition: • probe fitting check;
• stimulus calibration;
• acquisition itself.
38.
• Probe fittingcheck is an objective test of correctness of probe fitting in
external ear canal. It is done by analyzing the stimulus, recorded via probe’s
microphone.
• The acquisition window during this stage displays two linear scales: the one
is displaying the acoustic meatus volume (“volume” indicator appears
instead of reproducibility scale), and the other one is displaying the noise
level (“noise” indicator).
• If the noise level or the volume exceeds its respective threshold, the
corresponding scale becomes red, and if it does not, it stays green.
• If it is too noisy in the room, the acceptable noise level can be increased by
dragging the scale slider with the mouse.
• When the OAE probe is fitted correctly, both scales should be in the green.
39.
• If thesoftware detects that the OAE probe is fitted correctly, it will
switch to the next stage: stimulus calibration.
• Stimulus calibration is required for the accurate setting of the
specified stimulus intensity using the OAE probe’s built-in
microphone.
• The acquisition window always displays the specified and achieved
levels of stimulus intensity (in dB SPL).
40.
• TEOAE ACQUISITION-iscarried out in nonlinear mode. The sets of 4
stimuli are used in strict sequence – one large stimulus and three
small ones. During the acquisition the following information is
displayed:
Number of averaged and rejected traces (artifacts).
Stimulus stability. The ideal variant is when it is equal to ”1”.
The level of the averaged response, in dB SPL is opposite the “A&B”
label.
Total residual noise level, in dB SPL is opposite the “A-B” label.
“Reproducibility, %”. This value is the correlation between odd and
even traces of a signal.
41.
The table ofOAE presence by frequencies.
The top row, marked as “kHz”, contains 1, 2, 3, 4 and 5 kHz frequencies.
The middle row, marked as “SNR”, displays the current signal-to-noise
ratio on the given frequency (in dB), calculated with the use of the digital
bandpass filter.
The OAE presence on the given frequency is marked by “ ”symbol. The
criterion of its presence is specified in TEOAE settings (by default, 6 dB is
for adults and 4 dB – for newborns).
High correlation between A and B traces indicates OAE presence, and the
subtracted trace (A-B) helps to calculate the residual noise level. The
response spectrum has two areas: the dark one shows the noise level
and the light one indicates the response level, in those areas where it
exceeds the noise level.
DISTORTION PRODUCT EMISSIONS
•Distortion product otoacoustic emission (DPOAE) is an acoustic
response generated by patient’s cochlea when provided with two-
tone stimulation.
• As well as TEOAE, DPOAE represents extremely weak acoustic
vibrations which can be recorded in external auditory canal by very
sensitive low-noise microphone.
• As a rule, DPOAE is detected in persons with normal hearing only.
45.
• The techniqueis rooted in spectrum analysis of activity recorded in
response to simultaneous stimulation by two tones - F1 and F2.
• F2 is a primary tone and F1 is a secondary one.
• During DPOAE acquisition the dependence of OAE intensity on
stimulation frequency (F2) is plotted on DP-gram.
• Noise level on each frequency is plotted on the graph as well. The
received information gives a true functional status of outer hair cells
from the base of cochlea up to its apex.
46.
• OAE PROBEFITTING CHECK- is an objective test of correctness of
probe fitting in external ear canal. It is done by analyzing the stimulus,
recorded via probe’s microphone.
• STIMULUS CALIBERATION- n is applied for precise setting of specified
stimulus intensity by using the OAE probe’s built-in microphone. As
well as during DPOAE acquisition, two continuous tones of different
frequencies (F1 and F2) are used as stimuli at this step.
• ACQUISITION ANALYSIS-
•For DPOAE acquisition a special OAE probe is used. This probe has built-in
miniature speakers and a microphone, which should be inserted into the
external auditory canal of a patient.
• During DPOAE acquisition two continuous tones (F1 and F2) are used as
stimuli. Primary tone frequency is always preset. And secondary tone
frequency (F1) is calculated by the following ratio: F2/F1 = 1.22.
• During the acquisition at one frequency the responses are averaged and
the signal and noise values in decibels are calculated by response spectrum.
• Distortion product level in decibels is calculated by response spectrum as
well. The frequency of distortion product (DP), where the maximum
response intensity (distortion product) is usually calculated by the following
formula:
DP = 2*F1 – F2.



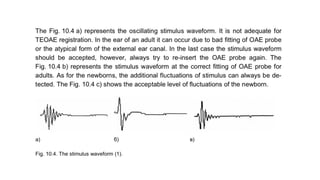
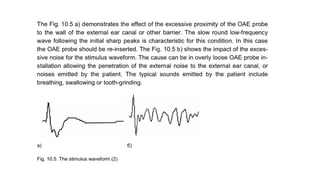

![Acquisition and analysis
• Start acquisition with repetitive stimulation using Acquisition|
Repetitive stimulation ([Ctrl+R]) menu command and follow the
process of signal averaging. To cancel the acquisition use Acquisition|
Cancel ([Esc]) menu command.
• To stop the stimulation for some time use Acquisition|Pause [space
key] menu command. The acquisition window is represented on Fig.
10.8.](https://image.slidesharecdn.com/malignantotitisexternalatest-250424194731-6a66de63/85/malignant-otitis-externa-diagnosis-and-management-35-320.jpg)