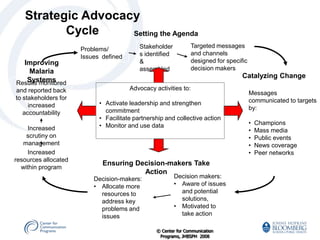
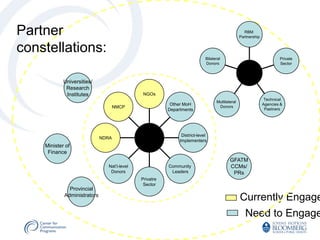
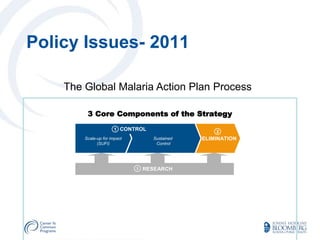
The document outlines a strategic approach to malaria advocacy, emphasizing the importance of targeted communication with decision-makers to increase resources for malaria control and treatment. It describes the advocacy process as collaborative and evidence-based, aiming to create motivation for resource allocation changes. Key components include building stakeholder consensus, monitoring results, and addressing challenges to ensure sustained impact and funding for malaria initiatives.
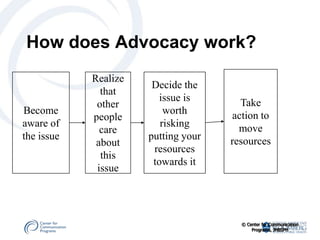








































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















