Downloaded 1,355 times











![SECOND PART – Deep to
hyoglossus, runs horizontally
forward along the upper border of
hyoid bone between hyoglossus
laterally and middle constrictor,
stylohyoid ligament medially.
THIRD PART [ ‘arteria profunda
linguae’ ]—Also called as deep
lingual artery.
-It runs upwards along the anterior
Border of hyoglossus, then
horizontally forwards on the
undersurface of tongue on each
side of frenum linguae.
-In vertical course,it lies b/t the
genioglossus medially & inferior
longitudinal muscle of tongue
laterally. Horizontal part is
accompanied by lingual nerve.](https://image.slidesharecdn.com/externalcarotidarterybranchesandligation-160303154214/75/External-carotid-artery-branches-and-ligation-22-2048.jpg)



![Cervical part : Cervical
part Runs upwards on
superior constrictor of
pharynx deep to the
posterior belly of
digastric.
-It grooves the posterior
border of
submandibular gland,
makes S-bend [2 loops]
1st winding down over
submandibular gland &
then up over the base
of mandible.](https://image.slidesharecdn.com/externalcarotidarterybranchesandligation-160303154214/75/External-carotid-artery-branches-and-ligation-27-2048.jpg)




























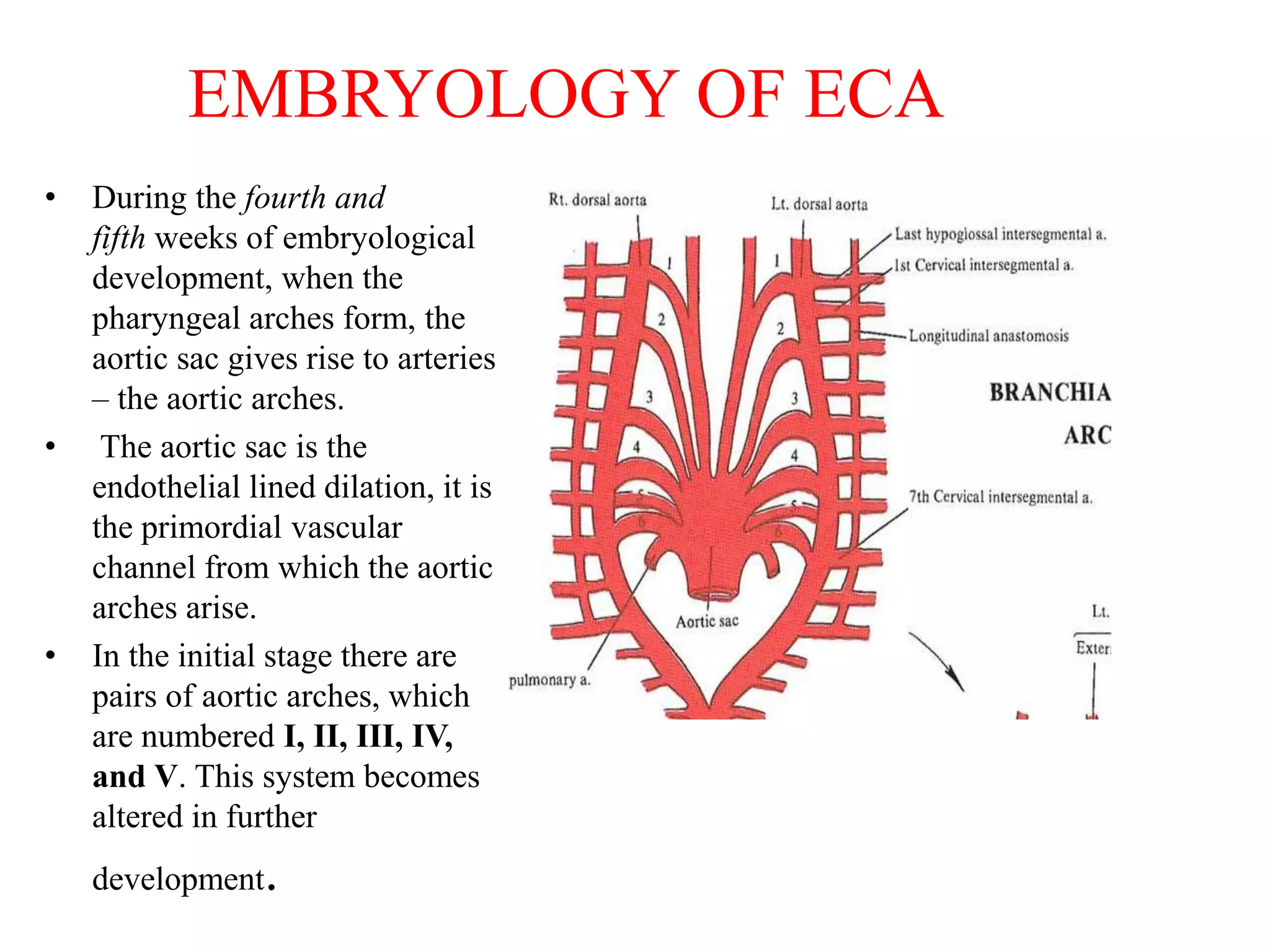
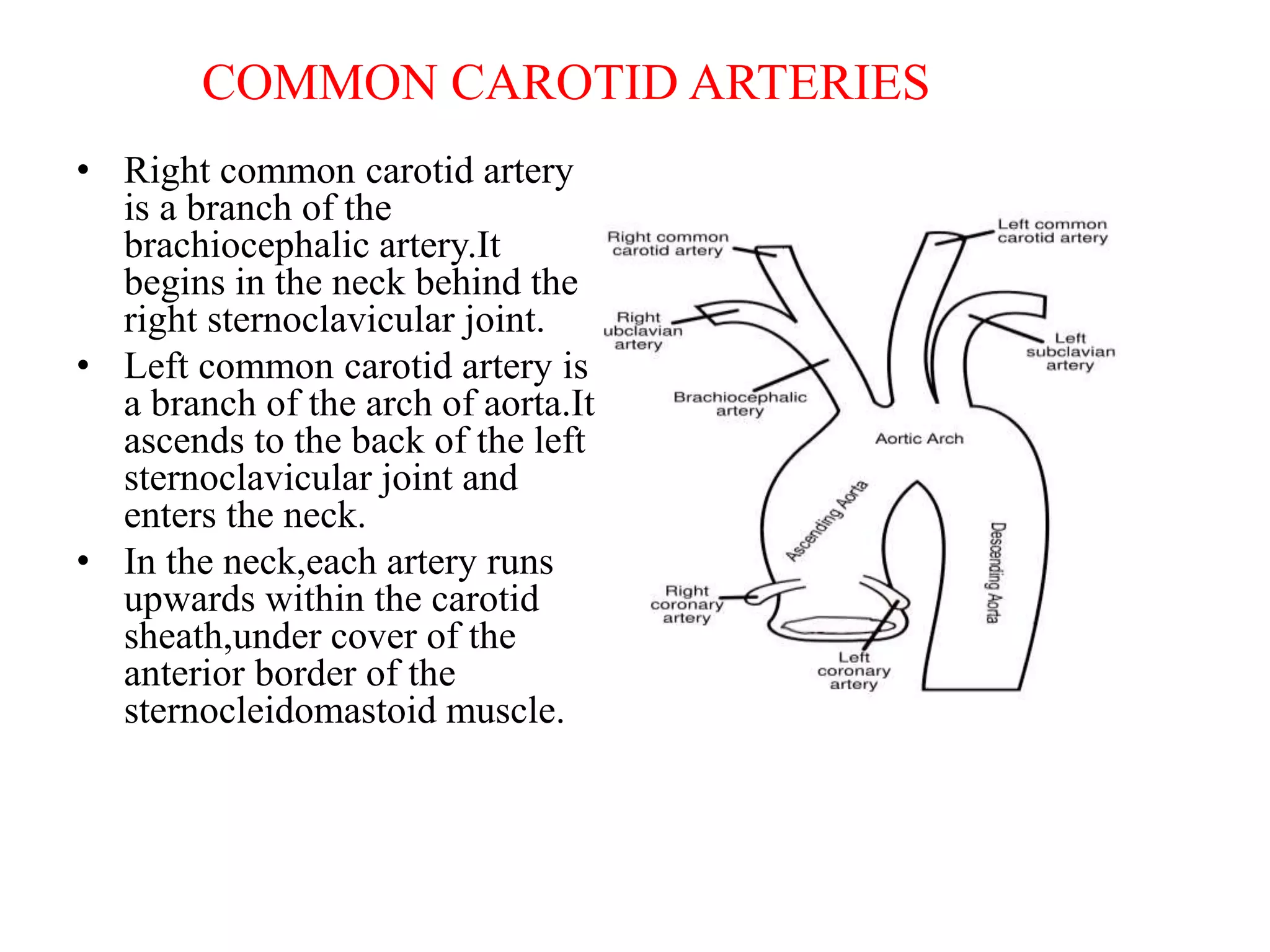
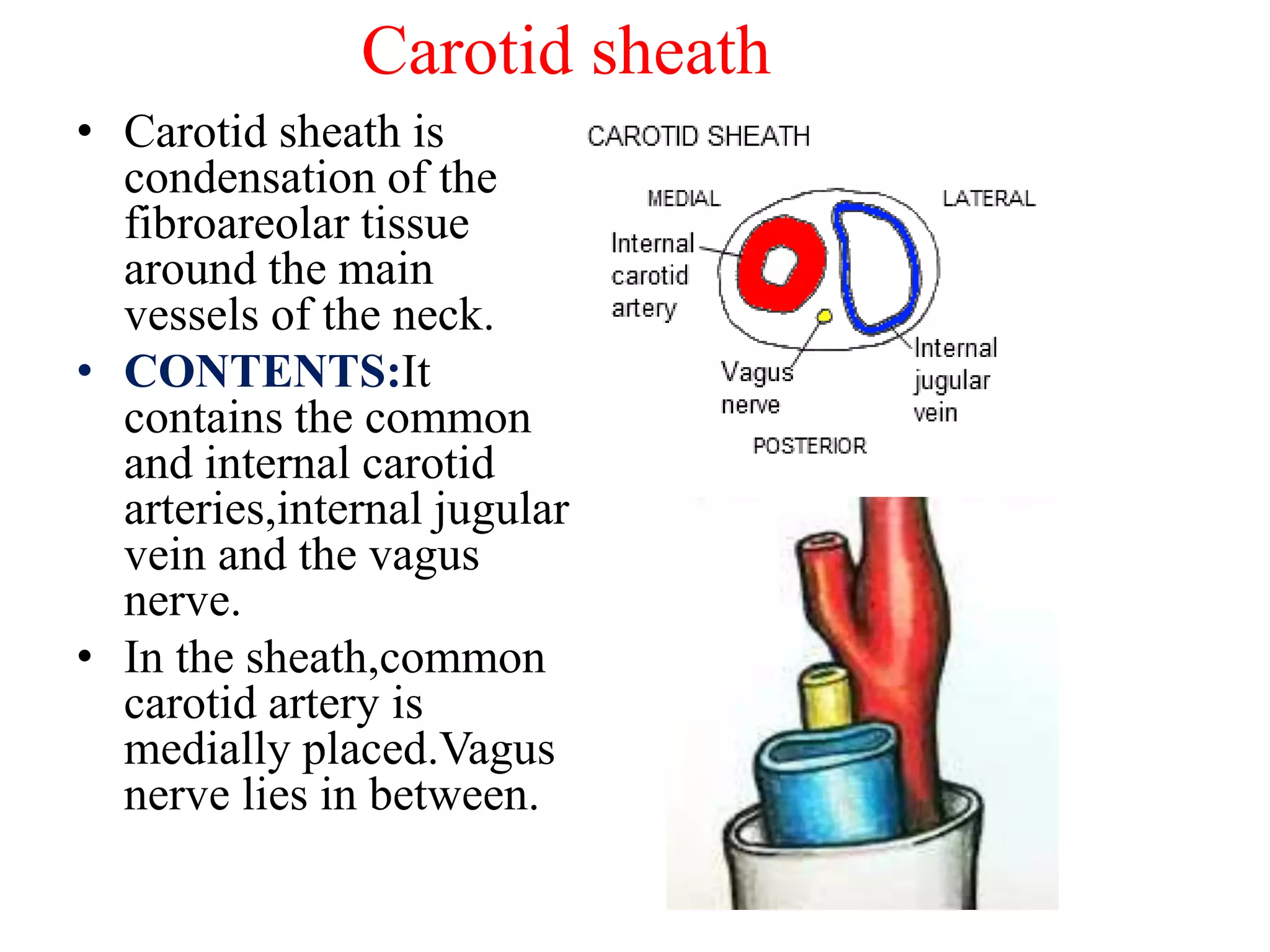
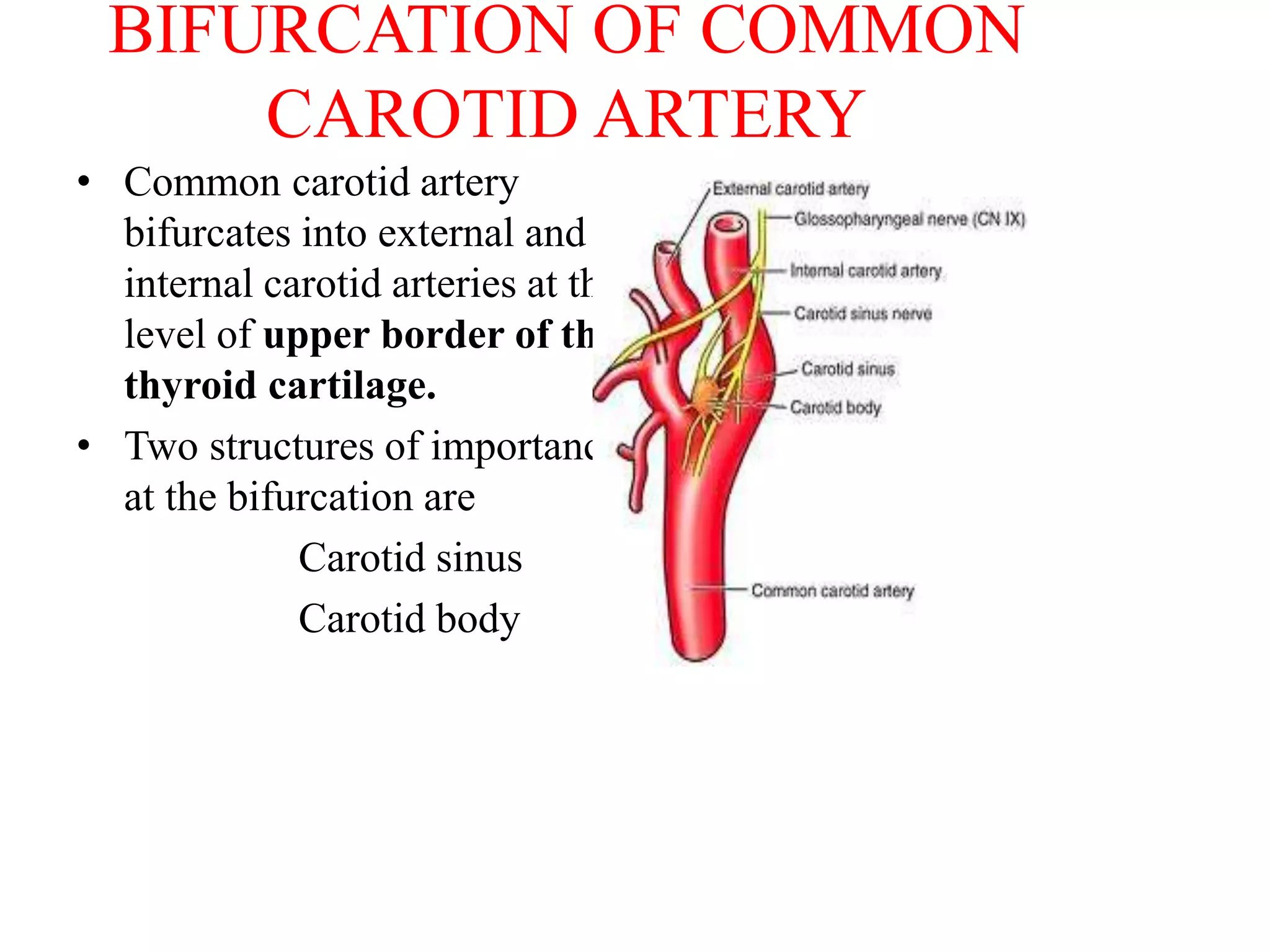
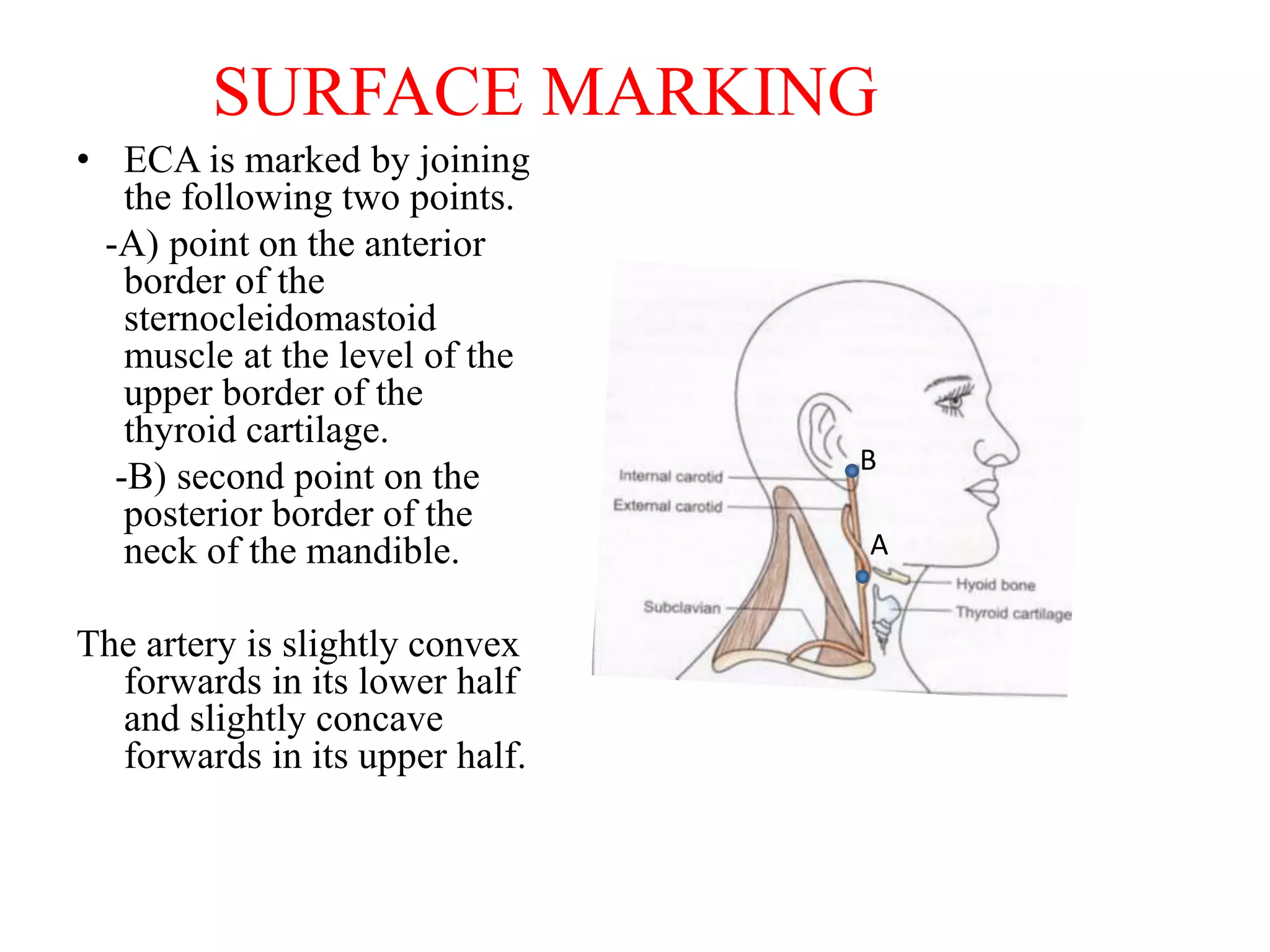
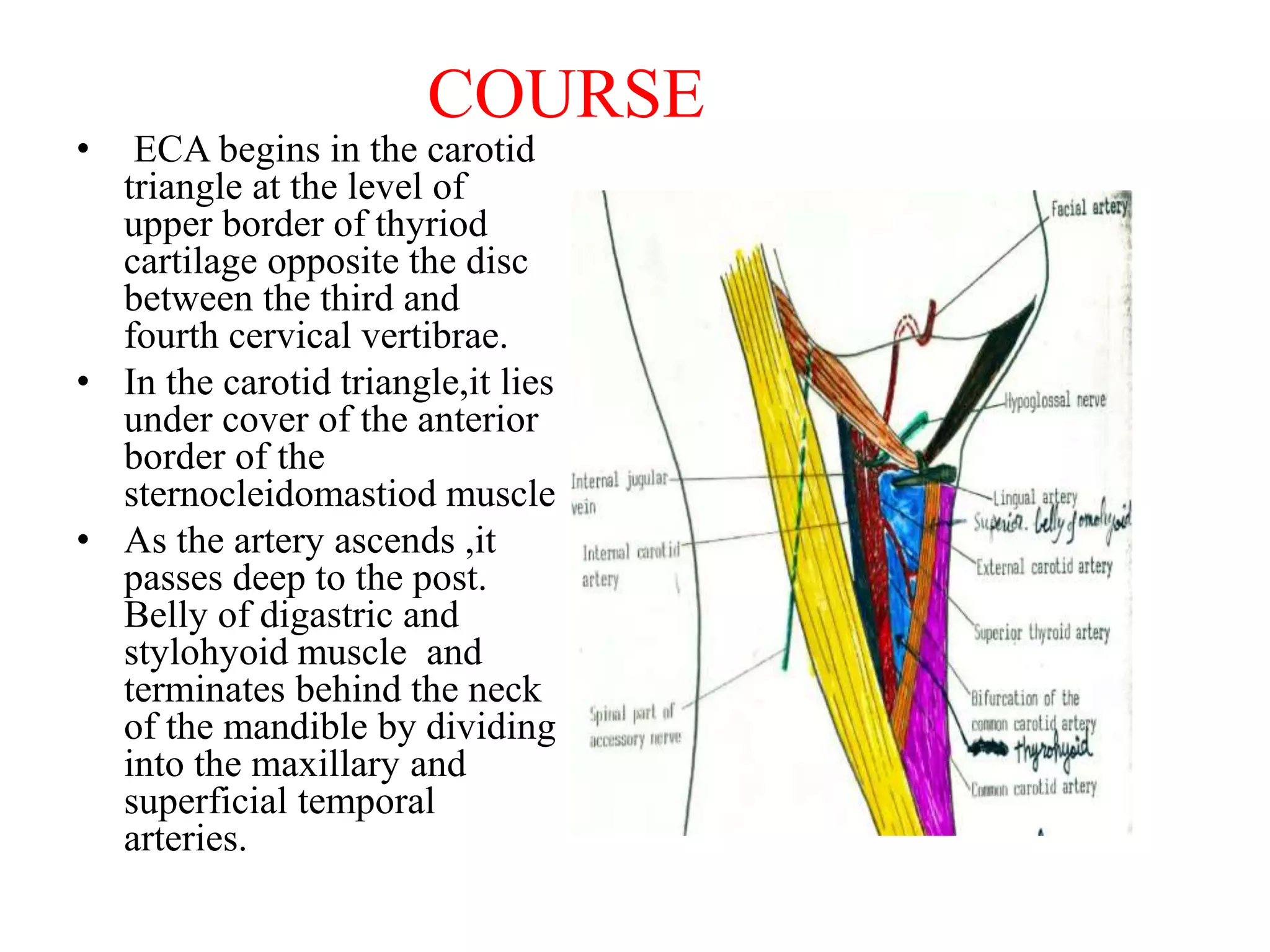
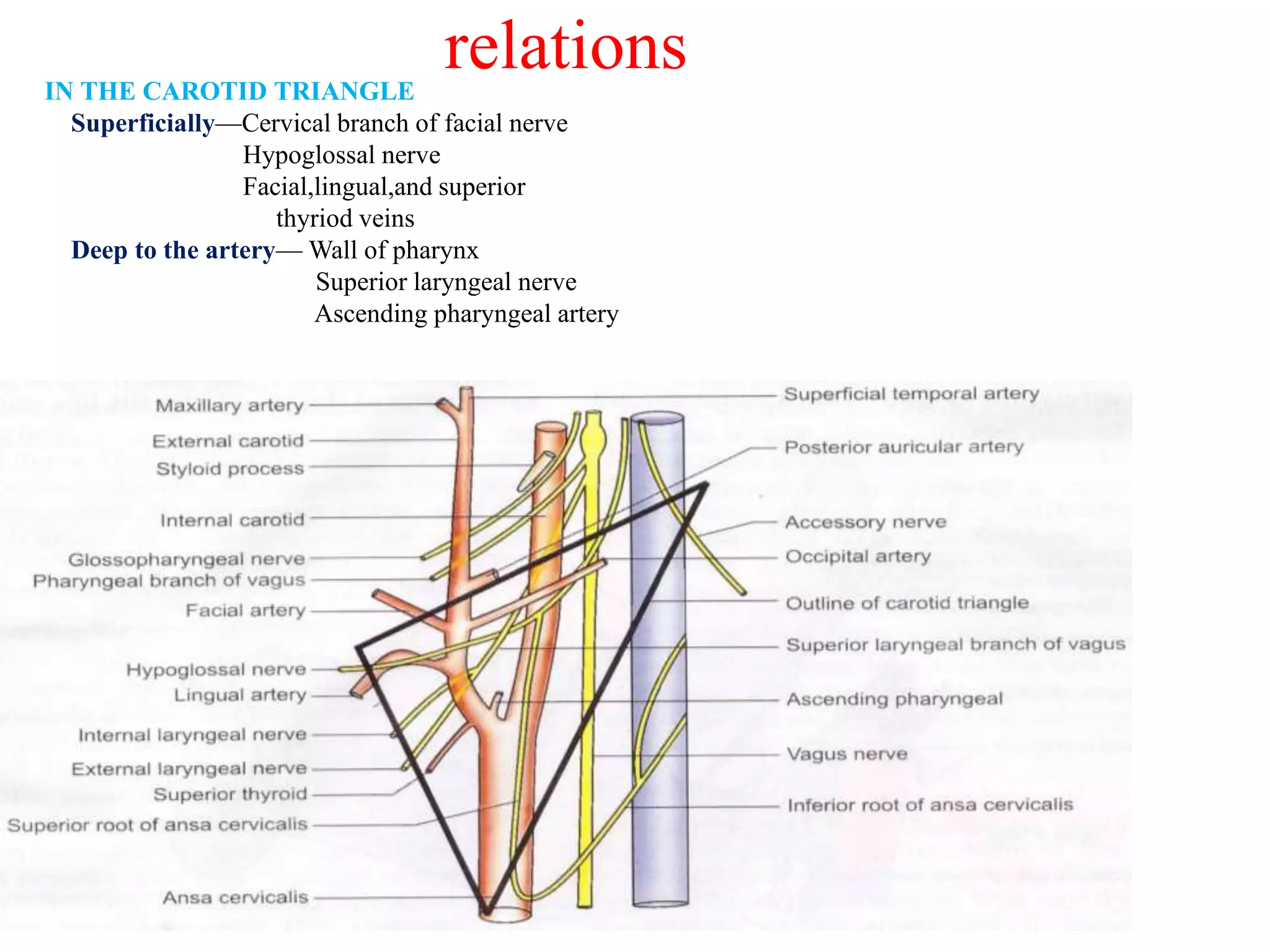
The document discusses the external carotid artery, its branches, and ligation. It begins with an introduction and overview of the embryological development of the external carotid artery. It then describes the common carotid arteries and their course in the neck. It discusses the bifurcation of the common carotid artery and structures located there - the carotid sinus and carotid body. The external carotid artery is then described in detail, including its course, branches, and relations. The branches discussed include the superior thyroid, lingual, facial, occipital, posterior auricular, ascending pharyngeal, maxillary, and superficial temporal arteries. Indications for ligation and surgical approaches are provided at the end.



































































