Downloaded 594 times
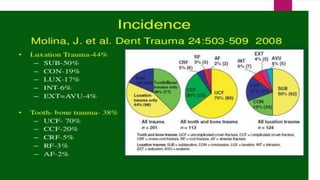
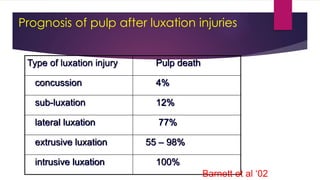

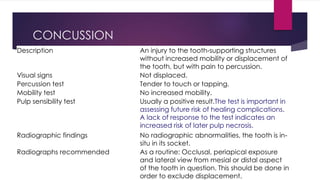
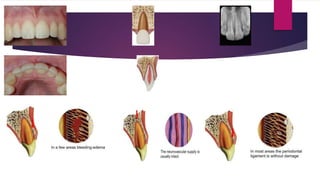
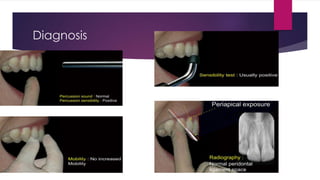
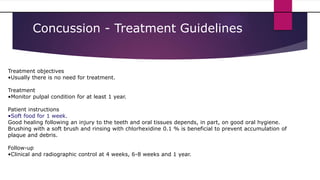

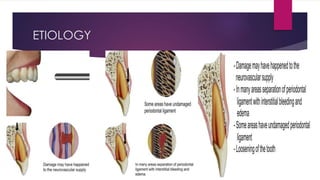
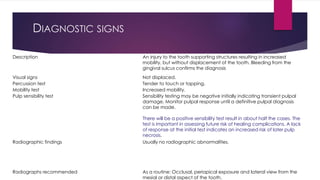
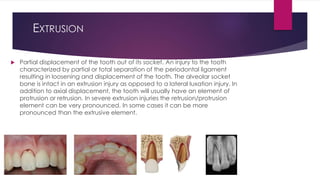
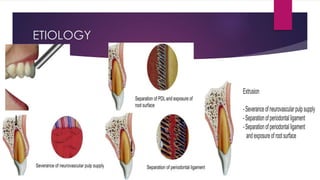
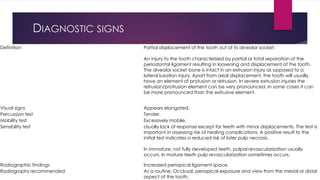
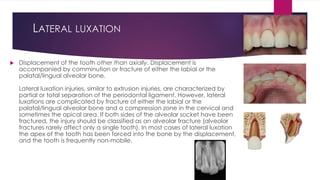
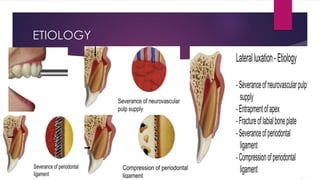
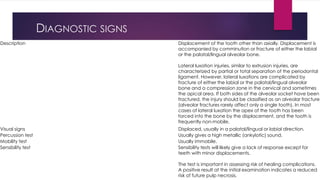

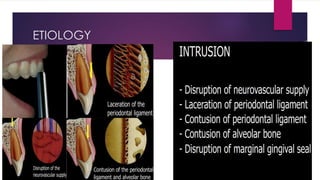
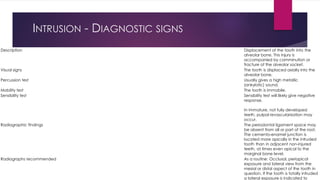

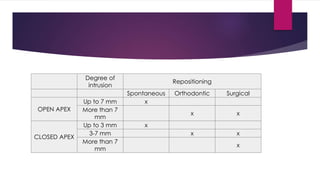
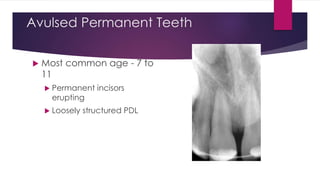
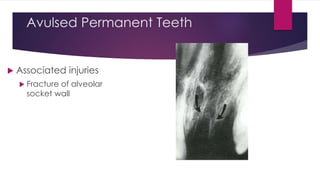
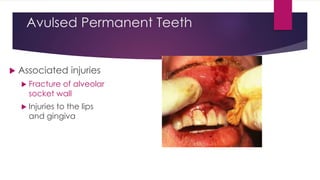
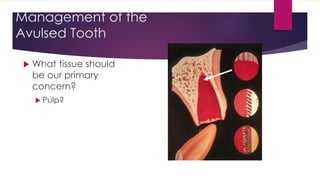
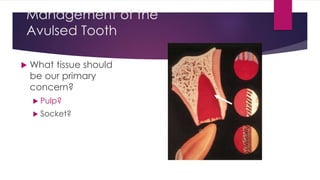
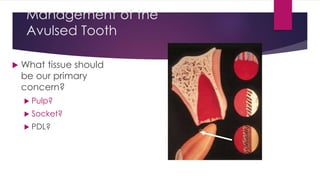
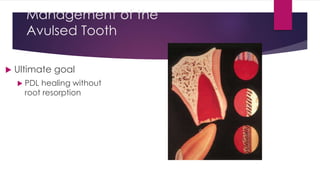
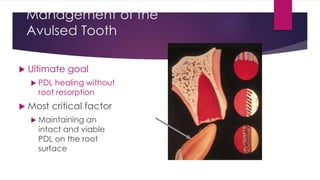










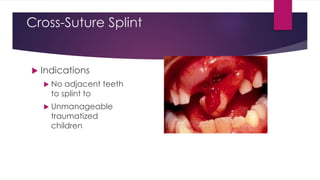


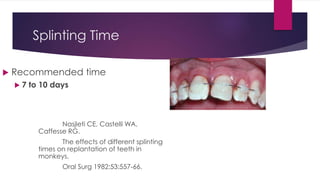
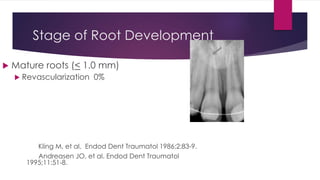



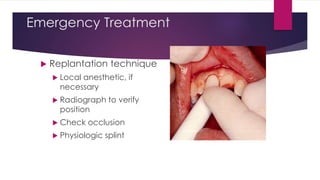





Luxation injuries involve displacement of teeth from their sockets and can range from mild concussions to complete avulsion. The document outlines the different types of luxation injuries including subluxation, extrusive luxation, lateral luxation, and intrusive luxation. It provides details on the diagnostic signs, treatment objectives, and prognosis for each type of injury. Pulp necrosis rates vary depending on the severity of the luxation, from 4% for concussions to 100% for intrusive luxations. Treatment generally involves repositioning the tooth, splinting for support, and monitoring for pulp necrosis over time.



































































