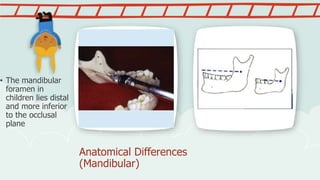
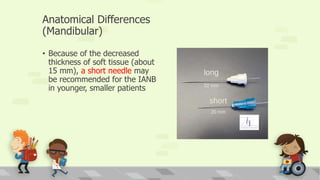
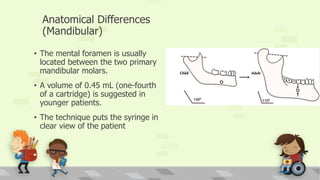
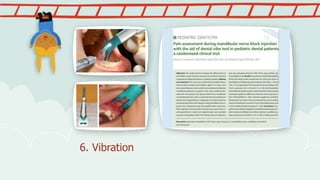
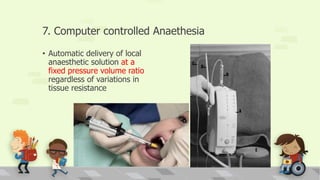
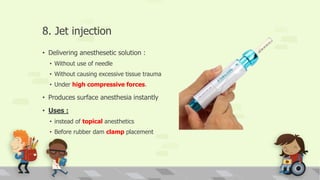
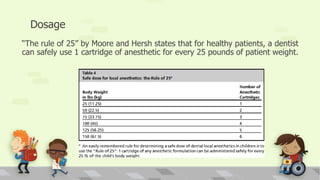
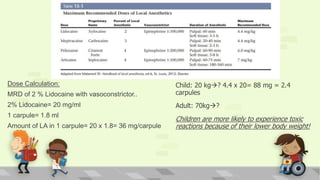
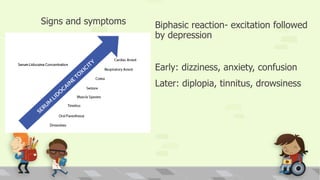
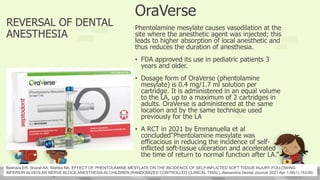
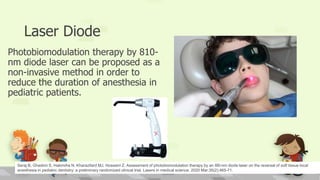
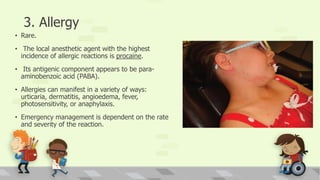
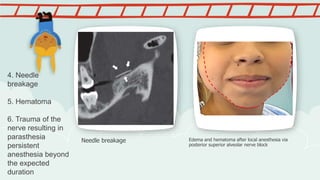
This document discusses local anesthesia techniques in pediatric dentistry. It begins by noting the importance of pain control for child behavior guidance. Anatomical differences between children and adults are described, including thinner bone and tissues in children, allowing for less needle penetration depth and smaller volumes of local anesthetic. Techniques for maxillary and mandibular anesthesia are outlined. Methods to minimize injection pain are provided, such as topical anesthetics, buffering or warming solutions, and vibration devices. The risks of toxicity, soft tissue trauma, allergic reactions and nerve damage are reviewed along with preventive measures. Reversal agents like OraVerse are also mentioned. Overall, the document provides an overview of best practices for safe and effective local


























![Local Anesthesia in childs [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/localanesthesiainchildsautosaved-240712192726-fceb4391-thumbnail.jpg?width=640&height=640&fit=bounds)














































