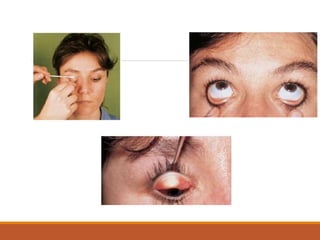
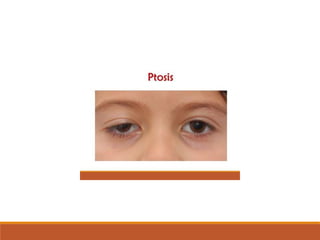
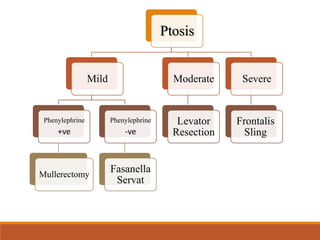
This document discusses the examination of eyelids and ptosis. It outlines how to inspect eyelid position, eversion of the upper eyelid, and demonstration of ptosis evaluation and surgery. Examination of the eyelids involves inspection of position, palpebral fissure width, and skin. History should include onset, duration, laterality, worsening, diplopia, weakness and trauma. Examination evaluates head posture, scars, laxity, telecanthus and epicanthus. Ptosis is measured by marginal reflex distance, vertical fissure height, levator function and lid crease level. Levator function classifies ptosis as mild, good, fair or poor. Decision making depends on