Downloaded 14 times
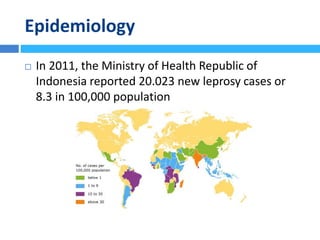
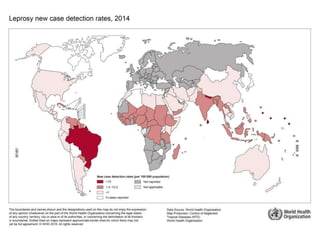
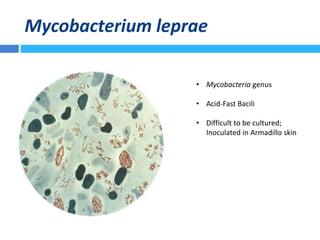
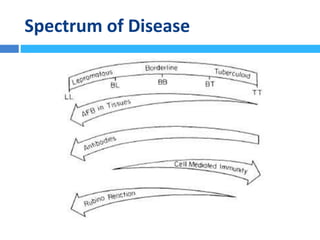
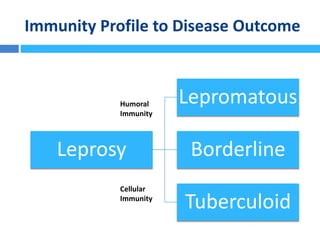

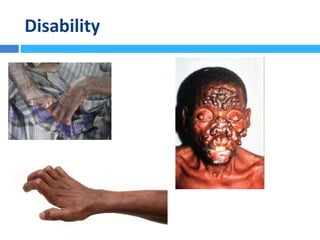
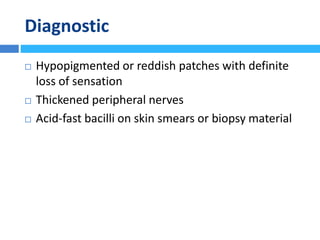
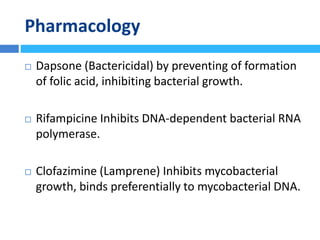

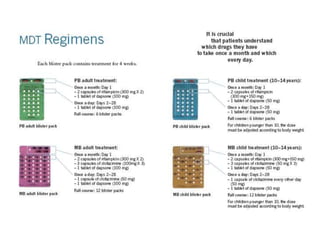

Leprosy, also known as Hansen's disease, is caused by the bacterium Mycobacterium leprae. It primarily affects the skin and nerves. Indonesia reported over 20,000 new leprosy cases in 2011. The disease has a spectrum, ranging from paucibacillary (PB) which involves fewer skin lesions and bacteria, to multibacillary (MB) with widespread lesions and high bacteria levels. Treatment involves multidrug therapy with dapsone, rifampicin, and clofazimine over 6-24 months depending on classification. While treatment can cure the disease, nerve and tissue damage may be permanent if untreated for too long.




























































































