Downloaded 157 times
![“In God we trust. All others [must] have data.”
Dr. Bernard Fisher, surgeon, chairman of NSABP 3](https://image.slidesharecdn.com/namratalandmarktrials1-230304060913-4bcb7f7c/75/Landmark-trials-in-breast-cancer-pptx-3-2048.jpg)

















![Bartelink H, Maingon P, Poortmans P, et al. Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year
follow-up of a randomised phase 3 trial [published correction appears in Lancet Oncol. 2015 Jan;16(1):e6]. Lancet Oncol. 2015;16(1):47-56.
EORTC trial
Whole breast irradiation with or without boost
Lancet Oncology, 2015
Bartelink et al.
20 years follow-up
Question: How does a radiation boost following whole breast irradiation impact overall survival, local
control and fibrosis for early breast cancer patients?
Early breast cancer: Post BCS, pT1-2, pN0-1, M0 ◊ n = 5569
◊ Adjuvant chemotherapy when indicated
Early BC post lumpectomy, axillary dissection
Whole breast
irradiation
50 Gy/ 25 fractions/ 5
weeks
Whole breast irradiation (50
Gy/25 fractions) followed by
16 Gy/8 fractions boost
• Radiation boost improves local control (20
years cumulative: 16% in no boost versus
12% boost (more for younger age)
• No OS benefit
• Moderately increases severe fibrosis
• Can be avoided in women > 60 years
26](https://image.slidesharecdn.com/namratalandmarktrials1-230304060913-4bcb7f7c/75/Landmark-trials-in-breast-cancer-pptx-26-2048.jpg)




















![IBCSG 23-01
Lancet Oncology, 2013
Galimberti et al.
5 years follow-up
Galimberti V, Cole BF, Zurrida S, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised
controlled trial [published correction appears in Lancet Oncol. 2013 Jun;14(7):e254]. Lancet Oncol. 2013;14(4):297-305.
2001 ◊ RCT ◊ 931 patients
◊T1, T2 with clinically negative nodes ◊ 1 – 2 sentinel lymph node containing micro-metastases
◊ 90% received adjuvant chemotherapy, whole breast RT by tangents
Question: Is avoidance of axillary dissection non inferior to axillary dissection in patients with
one or more micrometastatic (<= 2 mm) sentinel lymph nodes and tumour <= 5 cm?
Post lumpectomy, adjuvant treatment
SLN Biopsy: 1 or 2 sentinel lymph nodes containing micro-
metastases
SLND
ALND
5 years DFS: No difference (87% in no AD
versus 84% in AD)
Toxicity: More cases of Grade 3-4 toxicity
(1 case of sensory neuropathy, 3
lymphedema, 3 motor neuropathy) in
ALND arm
Routine axillary dissection should be excluded in this subgroup of patients provided they receive
adequate adjuvant treatment
52](https://image.slidesharecdn.com/namratalandmarktrials1-230304060913-4bcb7f7c/75/Landmark-trials-in-breast-cancer-pptx-52-2048.jpg)




















![Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27 [published
correction appears in J Clin Oncol. 2008 Jun 1;26(16):2793]. J Clin Oncol. 2008;26(5):778-785. doi:10.1200/JCO.2007.15.0235
NSABP B18, B27
JCO, 2008
Rastogi et al.
Update of the two trials
Question: NSABP 18: How does addition of 4
cycles of AC preoperatively compare with
adjuvant AC?
NSABP B27: What is the effect of addition of
docetaxel to AC preoperatively?
Preoperative therapy = adjuvant therapy
B-27: Addition of preoperative taxanes to AC improves response compared with only AC
NSABP B18: Neoadjuvant AC is equivalent to adjuvant AC in terms of DFS, OS
NSABP B27: Preoperative T added to AC significantly increased pathologic complete responses (pCRs) compared with preoperative
AC alone (26% vs 13%)
*patients with pCR have significantly better OS, DFS than those who did not
73](https://image.slidesharecdn.com/namratalandmarktrials1-230304060913-4bcb7f7c/75/Landmark-trials-in-breast-cancer-pptx-73-2048.jpg)



































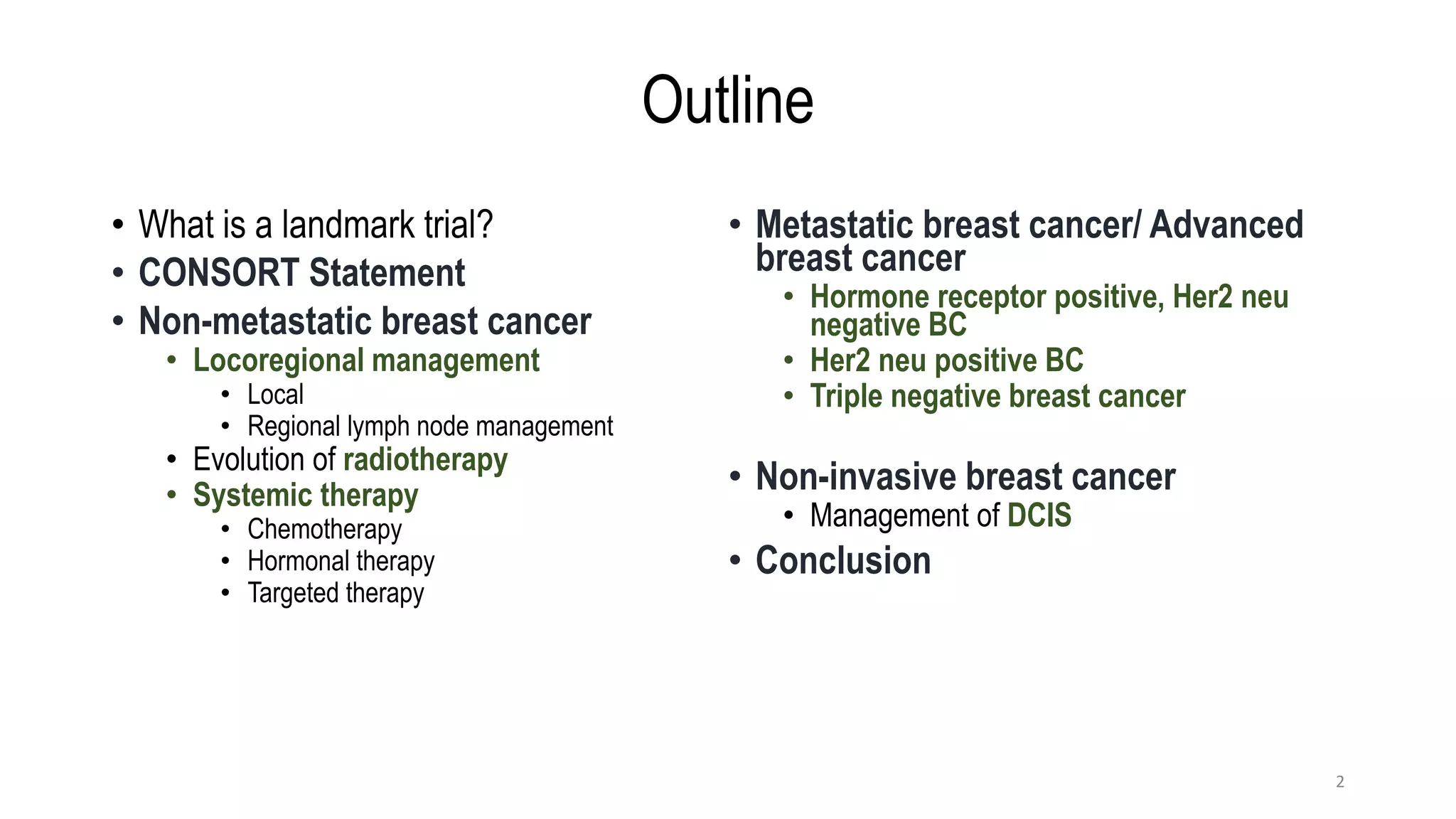
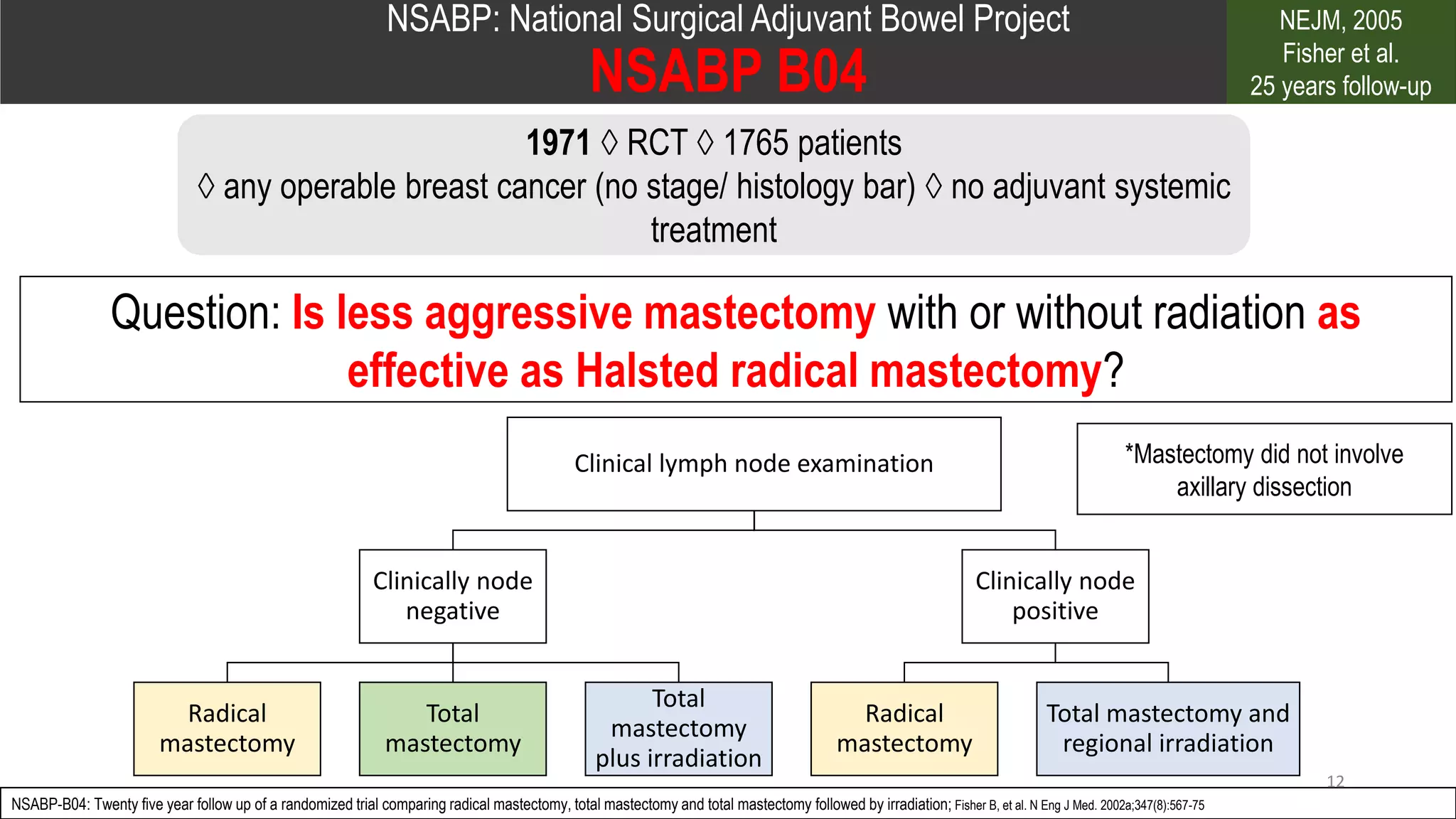
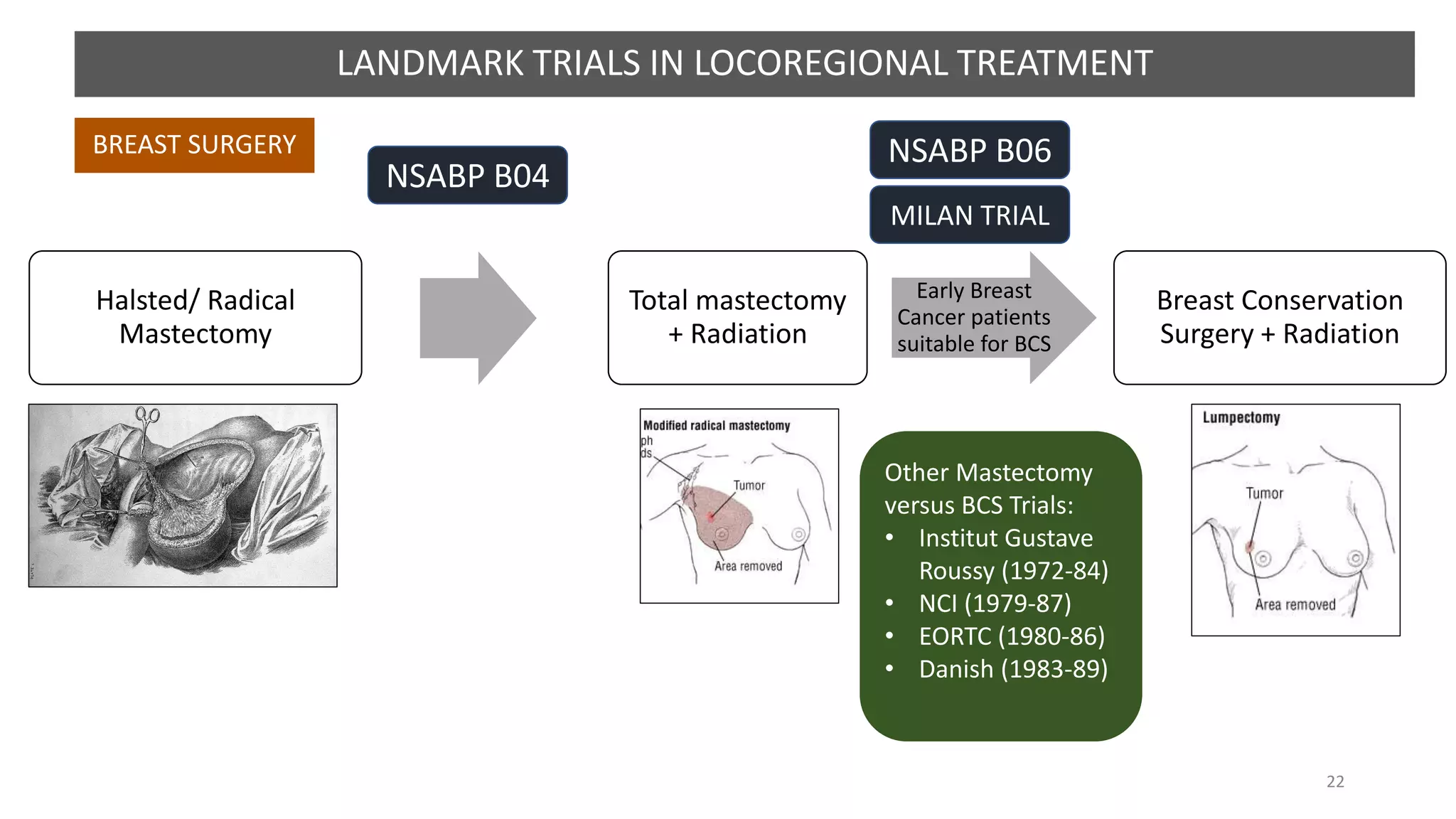
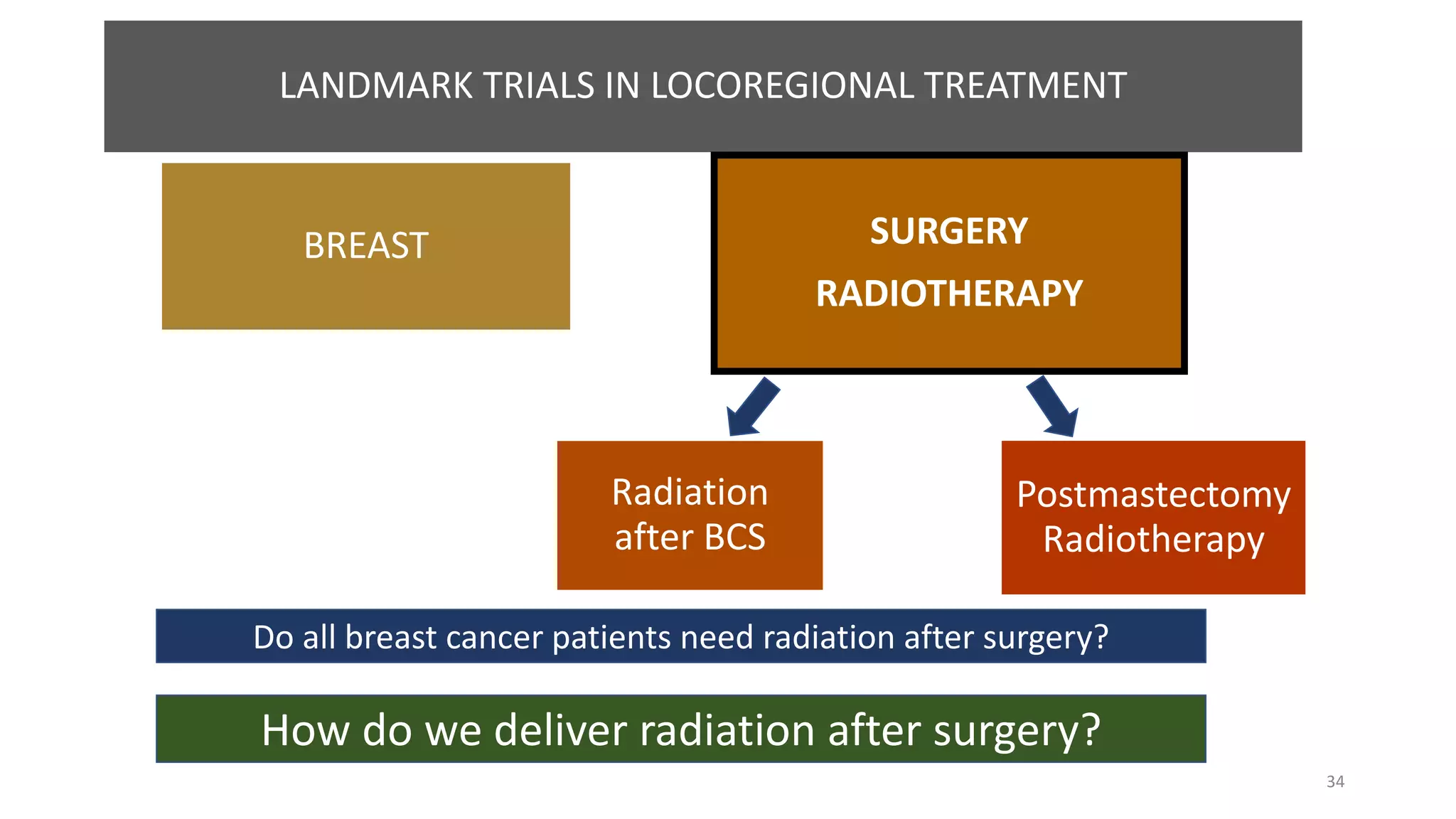
The document discusses landmark trials in the treatment of breast cancer, focusing on various management strategies including locoregional and systemic therapies. It highlights the evolution of treatments, the significance of randomized controlled trials, and the results of notable studies such as NSABP B04, Milan trial, and NSABP B06, which compared different surgical and treatment approaches. The conclusion emphasizes that less aggressive treatments can be as effective as radical surgeries, with advances in radiotherapy improving patient outcomes.










































































