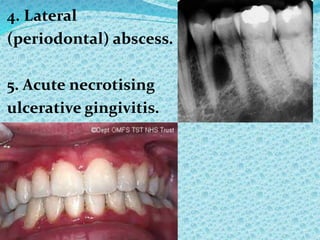
This document discusses orofacial pain and neuralgias. It defines pain and states that approximately 40% of the British population only visit dentists for pain relief. It then lists and describes various types of orofacial pain including those related to dental issues, jaw diseases, edentulism, postoperative issues, pain triggered by chewing, neurological diseases like trigeminal neuralgia, and atypical facial pain. It provides details on diagnosing and treating specific conditions like trigeminal neuralgia and Bell's palsy.


















![[061021] Frictional Keratosis.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/061021frictionalkeratosis-220731004211-9572abf2-thumbnail.jpg?width=640&height=640&fit=bounds)




























































































