Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era
•
3 likes•557 views

Robert Anders, MD, PhD, Julie R. Brahmer, MD, MSc, and Christopher D. Gocke, MD, prepared useful Practice Aids pertaining to immunotherapy and biomarker testing for this CME/MOC/CC activity titled "Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era." For the full presentation, monograph, complete CME/MOC/CC information, and to apply for credit, please visit us at http://bit.ly/2L7zlSy. CME/MOC/CC credit will be available until May 2, 2020.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era
Similar to Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era
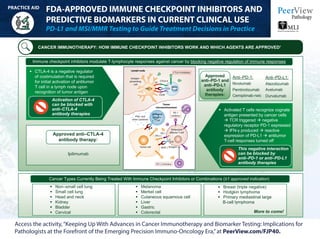
- 1. FDA-APPROVED IMMUNE CHECKPOINT INHIBITORS AND PREDICTIVE BIOMARKERS IN CURRENT CLINICAL USE PD-L1 and MSI/MMR Testing to Guide Treatment Decisions in Practice Access the activity,“Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era,”at PeerView.com/FJP40. PRACTICE AID CANCER IMMUNOTHERAPY: HOW IMMUNE CHECKPOINT INHIBITORS WORK AND WHICH AGENTS ARE APPROVED1 Immune checkpoint inhibitors modulate T-lymphocyte responses against cancer by blocking negative regulation of immune responses CTLA-4 is a negative regulator of costimulation that is required for initial activation of antitumor T cell in a lymph node upon recognition of tumor antigen Activated T cells recognize cognate antigen presented by cancer cells à TCR triggered à negative regulatory receptor PD-1 expressed à IFN-γ produced à reactive expression of PD-L1 à antitumor T-cell responses turned off This negative interaction can be blocked by anti–PD-1 or anti–PD-L1 antibody therapies Activation of CTLA-4 can be blocked with anti–CTLA-4 antibody therapies Approved anti–CTLA-4 antibody therapy: Anti–PD-1: Nivolumab Pembrolizumab Cemiplimab-rwlc Anti–PD-L1: Atezolizumab Avelumab Durvalumab Approved anti–PD-1 and anti–PD-L1 antibody therapies: Ipilimumab Cancer Types Currently Being Treated With Immune Checkpoint Inhibitors or Combinations (≥1 approved indication) Non–small cell lung Small cell lung Head and neck Kidney Bladder Cervical Melanoma Merkel cell Cutaneous squamous cell Liver Gastric Colorectal Breast (triple negative) Hodgkin lymphoma Primary mediastinal large B-cell lymphoma More to come! Lymph node Tumor microenvironment Antigen- presenting cell CTLA-4 inhibitor IFNγ and other cytokines Activated effector T cell PD-1 inhibitor B7 CD28 PD-L1 PD-1 MHC-I Antigen PD-L1inhibitor Tumor cell MHC-II CTLA-4 TCR TCR Exhausted effector T cell Naive T cell Treg cell
- 2. FDA-APPROVED IMMUNE CHECKPOINT INHIBITORS AND PREDICTIVE BIOMARKERS IN CURRENT CLINICAL USE PD-L1 and MSI/MMR Testing to Guide Treatment Decisions in Practice Access the activity,“Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era,”at PeerView.com/FJP40. PRACTICE AID PREDICTIVE TESTING: UNDERSTANDING THE DIFFERENCES BETWEEN COMPANION AND COMPLEMENTARY DIAGNOSTICS Specified on drug label Typically used when the test is among inclusion criteria for the trial (there are some exceptions) Test result is required for prescription of the drug Companion Complementary Test result is predictive, but not required for prescription of the drug Nice to have, but do not need to have Mostly used when the assay is integrated into the trial, but not used among inclusion criteria Predictive Diagnostic Categories: Companion vs Complementary PD-L1 Expression Testing PD-L1 is a ligand for the immune checkpoint receptor PD-1 expressed on the surface of cytotoxic T cells PD-L1 expression can be measured by IHC and detected on tumor and immune cells Optimal (IHC) Recent acquisition/current disease biopsy or resection Abundant tissue (area >25 mm2 , volume >1 mm3 ) Abundant tumor cells (>50% of nucleated cells) Proper fixation (12-24+ h in 10% NBF for cores) Fresh section from FFPE block (<3-5 days) Staining using a validated/approved assay Minimum (PD-L1) Within 36 months before treatment, any sample type Any tissue area (eg, >1-2 mm2 ) >100 viable tumor cells (22C3 and 28-8 pharmDx) Conventional fixation Sections obtained up to 2-3 months before staining Locally available and validated PD-L1 assay IMMUNO-ONCOLOGY BIOMARKERS: APPROVED PREDICTORS OF BENEFIT FROM CANCER IMMUNOTHERAPIES ü X
- 3. FDA-APPROVED IMMUNE CHECKPOINT INHIBITORS AND PREDICTIVE BIOMARKERS IN CURRENT CLINICAL USE PD-L1 and MSI/MMR Testing to Guide Treatment Decisions in Practice Access the activity,“Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era,”at PeerView.com/FJP40. PRACTICE AID IMMUNO-ONCOLOGY BIOMARKERS: APPROVED PREDICTORS OF BENEFIT FROM CANCER IMMUNOTHERAPIES (Cont’d) Immune Checkpoint Inhibitors and Associated PD-L1 Assays Nivolumab Pembrolizumab Atezolizumab Durvalumab Avelumab Target PD-1 PD-1 PD-L1 PD-L1 PD-L1 Antibody clone/ epitope 28-8 extracellular 22C3 extracellular SP142 cytoplasmic SP263 cytoplasmic 73-10 cytoplasmic IVD class III diagnostic partner Dako Dako Ventana Ventana Dako Scoring Tumor cells 1%, 5%, 10% TPS 1%, TPS 50%, CPS 10, CPS 1 10%/50%, Tumor/immune cells 5%, 1% Tumor cells 25% Tumor cells 1%, 50%, 80% Diagnostics Complementary (NSCLC, melanoma); PD-L1 IHC 28-8 pharmDx test Companion (NSCLC, bladder, gastric, cervical); PD-L1 IHC 22C3 pharmDx test Companion (bladder, TNBC) and complementary; Ventana PD-L1 (SP142) assay Complementary (bladder); Ventana PD-L1 (SP263) assay Unknown Setting Second line First line or second line First line or second line Second line Second line Bolding of text relates to companion diagnostic designation.
- 4. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. CPS: combined positive score; CTLA-4: cytotoxic T-lymphocyte–associated antigen 4; dMMR: deficient mismatch repair; IHC: immunohistochemistry; IVD: in vitro diagnostic; FFPE: formalin fixed paraffin embedded; mCRC: metastatic colorectal cancer; MMR: mismatch repair; MSI: microsatellite instability; MSI-H: microsatellite instability high; NBF: neutral buffered formalin; NGS: next-generation sequencing; PCR: polymerase chain reaction; PD-1: programmed cell death protein 1; PD-L1: programmed death-ligand 1; TCR: T-cell receptor; TNBC: triple-negative breast cancer; TPS: tumor proportion score. 1. Adapted from: Ribas A, Wolchock JD. Science. 2018;359:1350-1355. FDA-APPROVED IMMUNE CHECKPOINT INHIBITORS AND PREDICTIVE BIOMARKERS IN CURRENT CLINICAL USE PD-L1 and MSI/MMR Testing to Guide Treatment Decisions in Practice Access the activity,“Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era,”at PeerView.com/FJP40. PRACTICE AID IMMUNO-ONCOLOGY BIOMARKERS: APPROVED PREDICTORS OF BENEFIT FROM CANCER IMMUNOTHERAPIES (Cont’d) MSI/MMR Testing Microsatellite instability high or deficient mismatch repair (MSI-H/dMMR) status; indicators of genomic instability - MSI-H: Change in number of nucleotide repeats in DNA sequences à different number of repeats than in inherited DNA - dMMR: Loss of function in the MMR pathway, a key DNA repair system FDA-approved pan-cancer biomarker for pembrolizumab, and in mCRC, for nivolumab and nivolumab + ipilimumab Testing Methods for Determining MSI-H or dMMR Status Immunohistochemistry PCR + Capillary Electrophoresis NGS: Numerous assays being developed
- 5. TUMOR MUTATIONAL BURDEN AS AN EMERGING IMMUNO-ONCOLOGY BIOMARKER Rationale, Testing, and Harmonization PRACTICE AID Access the activity,“Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era,”at PeerView.com/FJP40. Mutations Neoantigens Immune system recognition of tumor TMB: What Is the Underlying Rationale for Using It as an Immuno-Oncology Biomarker?1-10 Abnormal activity in cellular pathways (eg, DNA damage repair, DNA replication) and exposure to mutagens (UV light, tobacco smoke) can ↑ the overall rate of somatic mutations in tumors Neoantigens TCR Neoantigen presentation Tumor cell Killer T cellDNA mutations HLA TMB represents an emerging IO biomarker TMB status correlates with outcomes in patients treated with immune checkpoint inhibitors across many tumors - TMB levels vary in different types of tumors; lung, skin, and bladder cancer represent high-TMB tumors, but % of many other cancers has been found to have high TMB also Often measured/reported as mutations per megabase (mut/Mb) Thresholds for high vs low TMB are still in flux and depend on assay and histology (various labs/groups may calculate it differently and include different kinds of mutations) Complementary to PD-L1 expression—appears to identify a distinct and independent population of patients ↑ in tumor-specific neoantigens → ↑ in # of tumor-infiltrating immune cells Activated & primed CD8+ cytotoxic T cells can recognize & target neoantigens that are peptide-bound to major histocompatibility complex class I & presented on tumor cells → anti-tumor immune response → tumor cell lysis
- 6. TUMOR MUTATIONAL BURDEN AS AN EMERGING IMMUNO-ONCOLOGY BIOMARKER Rationale, Testing, and Harmonization PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. IO: immuno-oncology; MSKCC: Memorial Sloan Kettering Cancer Center; NCI: National Cancer Institute; NGS: next-generation sequencing; TCGA: The Cancer Genome Atlas; TMB: tumor mutational burden; US FDA: United States Food and Drug Administration; WES: whole exome sequencing. 1. Hellmann MD et al. N Engl J Med. 2018;378:2093-2104. 2. Carbone DP et al. N Engl J Med. 2017:376;2415-2426. 3. Hellmann MD et al. Cancer Cell. 2018;33:843-852.e4. 4. Ramalingam S et al. American Association for Cancer Research Annual Meeting 2018 (AACR 2018). Abstract CT078. 5. Snyder A et al. N Engl J Med. 2014;371:2189-2199. 6. Rizvi NA et al. Science. 2015;348:124-128. 7. Le DT et al. N Engl J Med. 2015;372:2509-2520. 8. Van Allen EM et al. Science. 2015;350:207-211. 9. Hugo W et al. Cell. 2016;165:35-44. 10. Yarchoan M et al. N Engl J Med. 2017;377:2500-2501. 11. Chan TA et al. Ann Oncol. 2019;30:44-56. 12. https://www.focr.org/tmb. Accessed April 17, 2019. Access the activity,“Keeping Up With Advances in Cancer Immunotherapy and Biomarker Testing: Implications for Pathologists at the Forefront of the Emerging Precision Immuno-Oncology Era,”at PeerView.com/FJP40. TMB Harmonization Effort: Friends of Cancer Research12 Workflow Samples Publicly available TCGA data Cells derived from human tumors Clinical samples Analytical validation Clinical validation Goals Identify agreement between TMB calculated using WES and various targeted panels used in the clinic Agree upon creation of a universal reference standard using WES Identify agreement between TMB score from targeted panels and reference standard Conduct a retrospective analysis using patient outcome data to identify cutoff values and inform prospective studies Step 1: In silico analysis Step 2: Empirical analysis Step 3: Clinical analysis Timeframe May 2018 Spring 2019 Summer 2019 Participants: • 7 test developers • 6 pharmaceutical companies • US FDA • NCI • Academia Whole Exome Foundation NGS MSKCC NGS No. of genes ~22,000 324 cancer-related genes 468 cancer-related genes Coverage ~30 Mb 0.8 Mb 1.22 Mb Types of mutations Coding missense mutations Coding, missense, and indel mutations per Mb Coding missense mutation per Mb Germline mutations Subtracted using germline DNA Estimated bioinformatically and subtracted Subtracted using matched blood TMB definition Number of somatic, missense mutations in the tumor genome Number of somatic, coding mutations (synonymous and nonsynonymous), short indels per Mb of tumor genome Number of somatic, missense mutations per Mb of tumor genome Turnaround time At least 4-6 weeks 2 weeks 2 weeks TMB: Comparison of Select Assays11