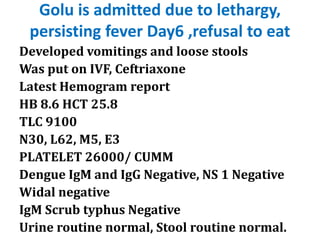
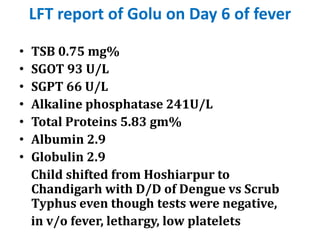
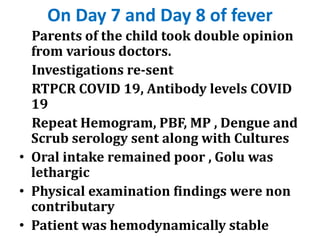
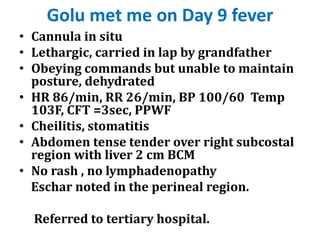
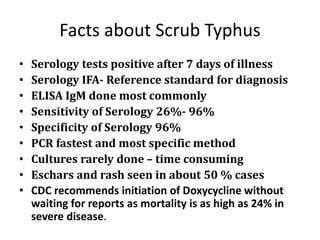
Golu, a 6-year-old boy, presented with a high-grade fever that persisted for 11 days, during which he experienced lethargy, vomiting, and low platelet counts. Despite negative tests for common infections such as dengue and scrub typhus, he was eventually diagnosed with scrub typhus on day 10 and deteriorated rapidly, leading to his tragic death. The case highlights the importance of thorough clinical evaluation and timely intervention in pediatric cases with fever and non-localizing symptoms.