Download to read offline



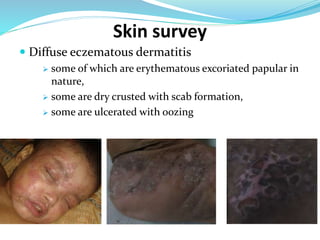




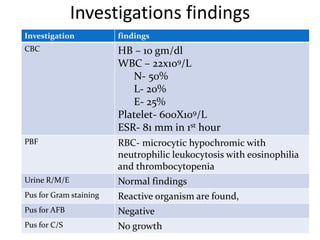
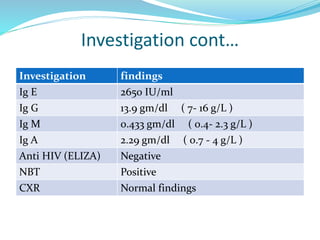


- A 5-year-old girl presented with a painful swelling on her right thigh that had been gradually increasing in size over the past month. She also had a history of recurrent skin lesions and infections since infancy. - On examination, she had diffuse eczematous lesions all over her body along with enlarged lymph nodes and ear discharge. Laboratory tests found elevated IgE levels. - The provisional diagnosis was primary immunodeficiency syndrome, likely Job's syndrome (hyper IgE syndrome) based on her recurrent skin and lung infections since infancy. She was treated with antibiotics and moisturizing cream.










































































