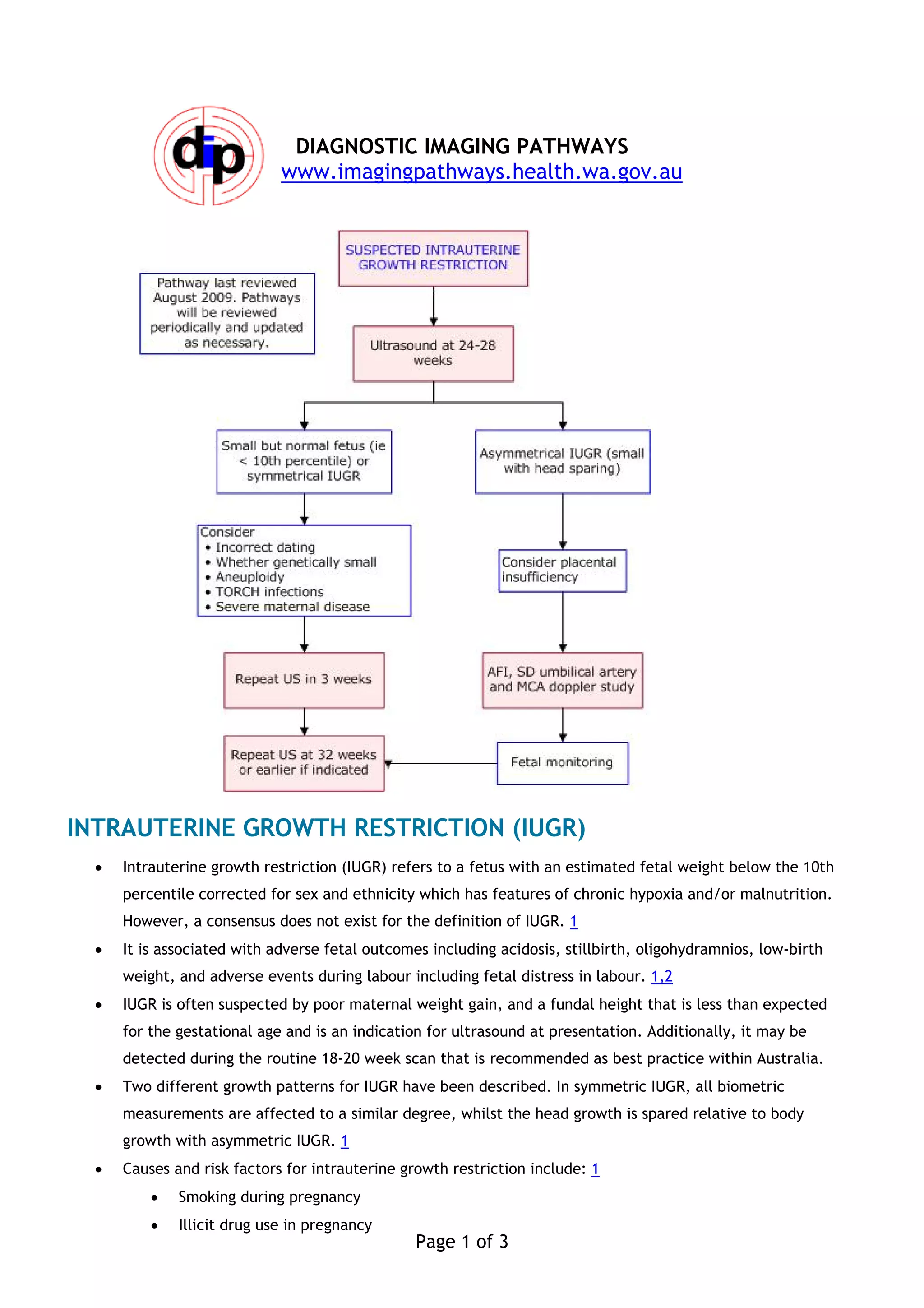
Intrauterine growth restriction (IUGR) refers to a fetus with an estimated weight below the 10th percentile. It can be suspected by poor maternal weight gain or a small fundal height, and is often detected on ultrasound. Causes include smoking, drugs, maternal health issues, and fetal abnormalities. Ultrasound assesses fetal anatomy, biophysical profile, and Doppler of the umbilical artery to evaluate blood flow. Abnormal Doppler readings correlate with adverse outcomes and help guide management. Serial ultrasounds may reduce emergency C-sections compared to cardiotocography alone for monitoring restricted growth fetuses.



















![Prediction and prevention of spontaneous preterm birth 2021 [votason.net]](https://cdn.slidesharecdn.com/ss_thumbnails/predictionandpreventionofspontaneouspretermbirth-2021votason-210822114401-thumbnail.jpg?width=640&height=640&fit=bounds)
















































