





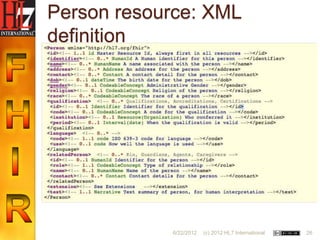
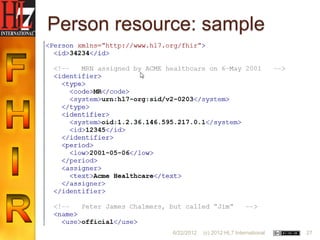
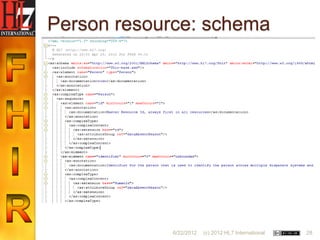
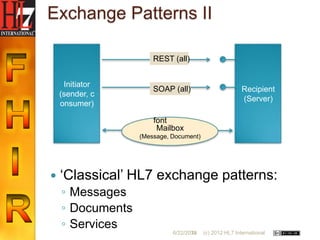


The document provides an introduction to FHIR (Fast Healthcare Interoperability Resources). It outlines some of the limitations of previous HL7 standards like V3 being too complex and documents (CDA) not being sufficient. It notes the need for a transition path from V2 and something to address new markets. FHIR is presented as a new approach that is focused on implementers and uses resources as the basic building block. Each resource has its own model and unique ID. The goal is to make implementation easier compared to previous standards.



























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














