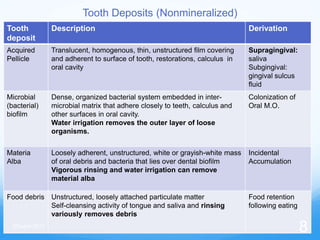
1. The document discusses soft deposits that form on teeth, including the acquired pellicle, dental biofilm, materia alba, and food debris.
2. The acquired pellicle is a translucent film that forms immediately after tooth cleaning from salivary glycoproteins. It allows for bacterial adhesion and calculus attachment.
3. Dental biofilm is a dense, non-mineralized mass of bacteria and other microorganisms embedded in a matrix. It develops in stages and can cause gingivitis if left undisturbed.