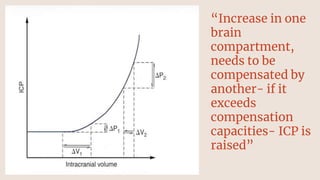
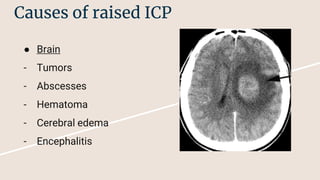
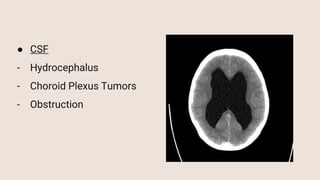
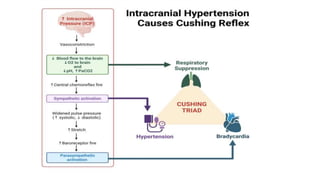
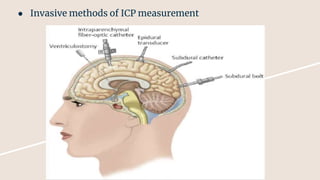
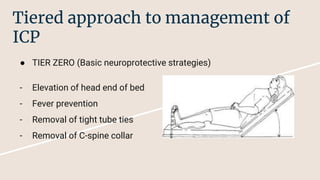
The document discusses intracranial pressure (ICP), its causes, identification methods, and management strategies. ICP increases when there is decompensation in cranial compartments due to factors like tumors, hydrocephalus, or vascular malformations. It outlines a tiered approach for management ranging from basic neuroprotective measures to advanced interventions like decompressive craniectomy.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













