Recommended
PDF
Case study : dengue fever
PPTX
PDF
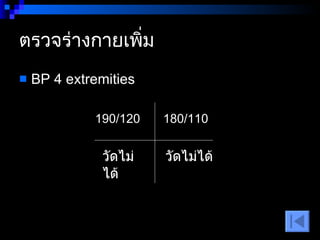
Basic mechanical ventilation sep 2552 with reference
PDF
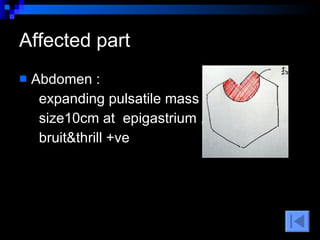
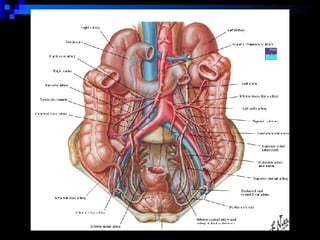
Risk matrix VS Risk profile
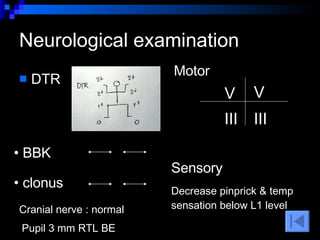
PDF
คำแนะนำการวินิจฉัยและการรักษาไข้เดงกีและไข้เลือดออกเดงกีในผู้ใหญ่ Rcpt 2013
PDF
Ch 8 basic emergency medical service and triage
DOC
คู่มือการจ่ายยาที่มีความเสี่ยงสูง
PDF
Pharmacotherapy in patient with stroke 2555
PDF
กลไกการคลอดปกติ 8 ขั้นตอน
PDF
SฺBAR เอสบา การสื่อสารอย่างปลอดภัย
DOC
การวัดความดันในหลอดเลือดดำกลาง Yui
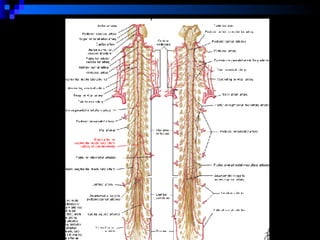
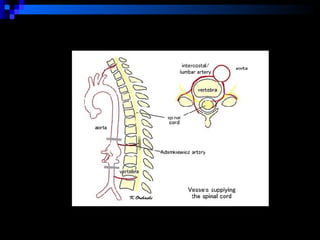
PPT
PDF
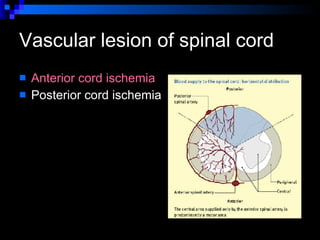
PDF
10 r กับการให้ยาอย่างปลอดภัย
PDF
Nursing Care for Coronary Artery disease edition 111058
PPTX
PDF
PDF
แนวทางการดูแลและจัดการความเจ็บปวดในเด็ก
PDF
PDF
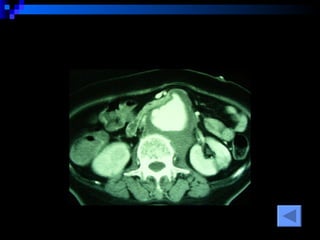
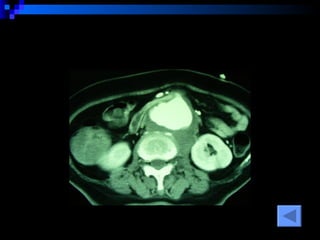
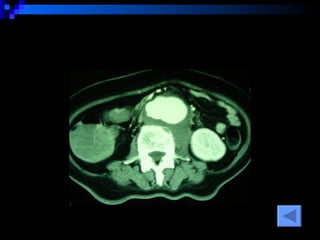
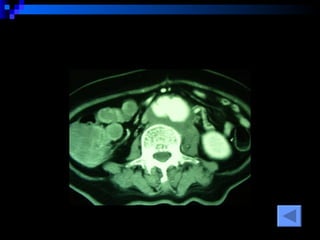
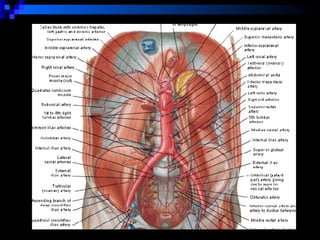
การให้สารละลายทางหลอดเลือดดำ
PDF
PPTX
อาการไม่พึงประสงค์จากยา ร้านยา
DOC
Central venous pressure (cvp)
PDF
12 กิจกรรมทบทวนภาคปฏิบัติ - Suradet Sriangkoon
PPT
Cvp central venous pressure monitoring
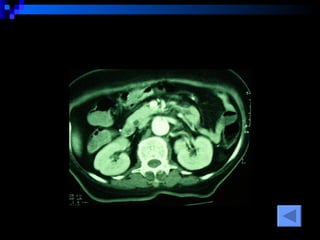
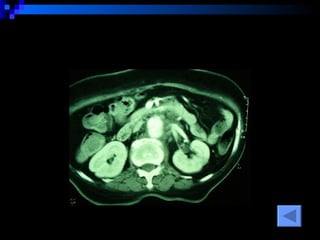
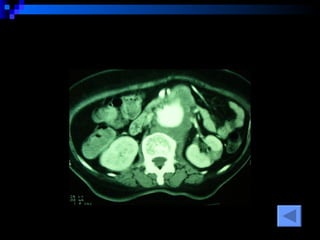
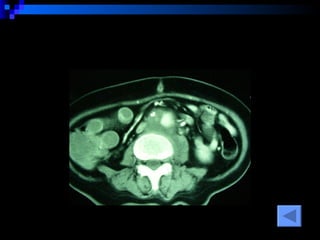
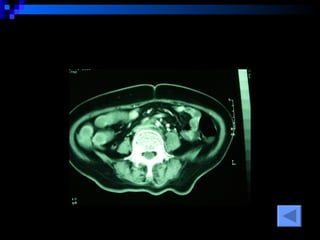
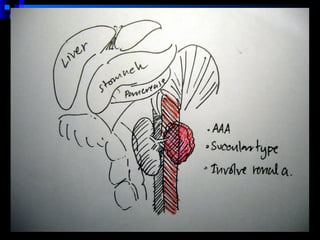
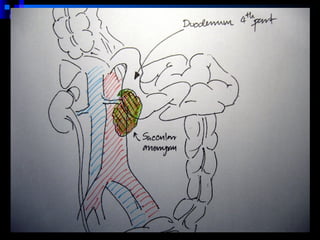
PDF
ภาวะสมองเสื่อม Clinical Practice Guidelines : Dementia
PDF
การดูแลผู้ป่วยที่ใช้เครื่องช่วยหายใจ
PDF
การดูแลผู้บาดเจ็บที่ทรวงอก
PPT
Common pitfalls in ER Procedure
PPT
Common pitfalls in Trauma
More Related Content
PDF
Case study : dengue fever
PPTX
PDF
Basic mechanical ventilation sep 2552 with reference
PDF
Risk matrix VS Risk profile
PDF
คำแนะนำการวินิจฉัยและการรักษาไข้เดงกีและไข้เลือดออกเดงกีในผู้ใหญ่ Rcpt 2013
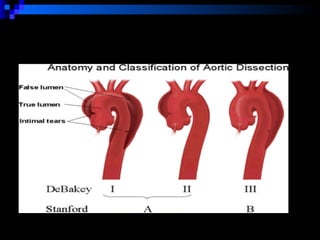
PDF
Ch 8 basic emergency medical service and triage
DOC
คู่มือการจ่ายยาที่มีความเสี่ยงสูง
PDF
Pharmacotherapy in patient with stroke 2555
What's hot
PDF
กลไกการคลอดปกติ 8 ขั้นตอน
PDF
SฺBAR เอสบา การสื่อสารอย่างปลอดภัย
DOC
การวัดความดันในหลอดเลือดดำกลาง Yui
PPT
PDF
PDF
10 r กับการให้ยาอย่างปลอดภัย
PDF
Nursing Care for Coronary Artery disease edition 111058
PPTX
PDF
PDF
แนวทางการดูแลและจัดการความเจ็บปวดในเด็ก
PDF
PDF
การให้สารละลายทางหลอดเลือดดำ
PDF
PPTX
อาการไม่พึงประสงค์จากยา ร้านยา
DOC
Central venous pressure (cvp)
PDF
12 กิจกรรมทบทวนภาคปฏิบัติ - Suradet Sriangkoon
PPT
Cvp central venous pressure monitoring
PDF
ภาวะสมองเสื่อม Clinical Practice Guidelines : Dementia
PDF
การดูแลผู้ป่วยที่ใช้เครื่องช่วยหายใจ
PDF
การดูแลผู้บาดเจ็บที่ทรวงอก
Viewers also liked
PPT
Common pitfalls in ER Procedure
PPT
Common pitfalls in Trauma
PPTX
Child Abuse Reporting Guidelines: Ethical and Legal Issues
PPT
PPT
PPT
Emergency Obstertrics & Gynecology
Similar to Interesting case
PPTX
Common surgical condition at opd for nurses
PDF
Interesting case ACLS.pdf
PPTX
2010_PMC Cardiovascular-Blood Disorder
DOC
การดูแลผู้ป่วยแน่นหน้าอก สงสัย Ischemiaxxx
PDF
PPT
การดูแลผู้ป่วยที่มีปัญหาโรคหัวใจ หลอดเลือด และ อัมพาต
PDF
PDF
PPTX
PPT
TAEM10:Emergency chest pain
PDF
Hemorrhagic shock 15 พค.2558
PPTX
ortho conference 3 nov 2017
PPTX
Guideline For the Early Management Of Patients with ischemic Stroke
PPTX
Ischemicstrokeyaya 140908125834-phpapp02
PPT
PPT
PDF
National license 2010 by med tu 16
PDF
National license 2010 by med tu 16
PDF
Motor weakness and Cerebrovascular Disease
PPTX
colles' fracture case dicussion
More from Narenthorn EMS Center
PDF
First aid by Narenthorn 2016
PDF
CPR2015 update: ACS and Special circumstances
PDF
PDF
CPR2015 update: Adult ACLS
PDF
PPTX
Neonatal resuscitation 2015
PPTX
CPR2015 update: BLS, CPR Quality and First aid
PPT
CPR2015 update: Ethical issues
PDF
การอำนวยความสะดวกการจราจรระหว่างการซ้อมแผน
PDF
Acute coronary syndrome 2010
PDF
Team dynamic for Advanced life support checklist
PDF
PDF
PDF
Trauma Initial assessment and Resuscitation
PDF
PDF
DOC
การยกและการเคลื่อนย้ายผู้ป่วย
PDF
Neonatal resuscitation การช่วยฟื้นชีวิตทารกและทารกแรกเกิด
PDF
Airway workshop Reading material
PDF
APHLS & EMS director 2011 Exam
Interesting case 1. 2. INTERESTING CASE ผู้ป่วยหญิงไทย อายุ 52 ปี CC : ขาอ่อนแรงสองข้าง 2 ชั่วโมงก่อนมารพ . PI : 2 ชั่วโมงก่อนมารพ . หลังตื่นนอนตอนเช้า มีอาการชาขา ขยับขาไม่ได้ ลุกไม่ขึ้น ไม่เจ็บอก ปวดหน่วงท้องน้อย ร้าวไปขา ปวดหลัง ต่อมา 1 ชั่วโมง ผู้ป่วยมีอาการอาเจียนเป็นเลือดสด 1 ครั้ง ประมาณครึ่งแก้ว ( 50 cc ) ไม่มีถ่ายดำ ไม่มีถ่ายเป็นเลือด ไม่หน้ามืด 3. PAST HISTORY Underlying HT poor control Underlying โรคกระเพาะอาหาร เป็นๆหายๆ ทานยาหม้อเป็นประจำเนื่องจากปวดหลังบ่อยๆ ดื่มสุราวันละ 1 แก้ว หยุดมา 3 เดือน สูบบุหรี่วันละ 1 ซอง หยุดมา 3 เดือน 4. 5. Physical examination V/S BT 36.5 PR 150 RR 20 BP 190/120 Moderate pale , no icteric sclera Lung : clear Heart : tachycardia ,regular ,no murmur Abdomen : ill-defined mass at epigastrium , voluntary guarding , rebound –ve No sign chronic liver disease 6. 7. Abdomen : expanding pulsatile mass , size10cm at epigastrium , bruit&thrill +ve Affected part 8. Neurological examination DTR clonus Cranial nerve : normal Pupil 3 mm RTL BE Motor V V III III BBK Sensory Decrease pinprick & temp sensation below L1 level 9. 10. Pulse Pulse examination Rt Lf Carotid 2+ 2+ Radial 2+ 2+ Femoral 0+ 0+ Popliteal 0+ 0+ Posterior tibial 0+ 0+ Dorsalispedis 0+ 0+ Cyanosis of distal toes & cold skin 11. 12. 13. 14. 15. 16. Problem list Acute paraparesis Acute limb ischemia UGIH Abdominal pulsatile mass Malignant HT Underlying PU 17. 18. 19. 20. Appraoch weakness UMNL อ่อนแรงเป็นกลุ่มๆ , ครึ่งซีก หรืออาจ 2 ข้างก็ได้ hypertonia, spasticity DTR ไว BBK, clonus + No fasciculation LMNL อ่อนแรงเฉพาะมัด หรือเป็นกลุ่ม Hypotonia or flaccid DTR – BBK, clonus – Fasciculation 21. UMNL weakness ถ้ามี cranial nerve involvement ให้ดูว่า cranial involve ข้างเดียวกันหรือคนละข้างกับแขนขาที่ weak ถ้าคนละข้าง brainstem , ถ้าข้างเดียวกัน อาจเป็นได้ทั้ง cortex และ subcortex ถ้าไม่มี cranial involvement และมี sensory loss เป็น level spinal cord lesion 22. Spinal cord lesion : causes Acute Vascular : dissection , emboli Rupture AVM Trauma Subacute/chronic Infection : staph, fungus , TB Tumor HNP Vasculitis 23. 24. Anterior spinal cord ischemia Radicular pain at onset Sudden paraplegia Flaccid spastic Areflexia hyperreflexia and extensor plantar response Loss pain , temp Preserved vibration & joint position Bowel & bladder symptoms 25. 26. 27. Management Airway : หายใจได้เอง , no airway obstruction Breathing : หายใจเร็วเล็กน้อย , O2 sat 99% (O2 canula 3 LPM) , equal BS Circulation : severe HT At 10.30 BP 262/155 , PR 131 , RR 24 Propanolol (40) 1 tab oral stat Then NTG (1:10) 5 ud/min 10 ud/min 28. Management NPO , retained NG tube 0.9% NaCl 1000 ml iv KVO x 2 เส้น omeprazole 40 mg iv q 12 hr G/M PRC 6 unit Monitor EKG BP q ½ hr Hct q 4 hr 29. 30. CBC 7.8 23.7 24,600 N=70 L=25 280,000 Coag : PT 12.7 (ratio 1.08 ) Ptt 25.1 (RATIO 0.84 ) Tt 6.3 ( RATIO 0.9) 31. 32. LFT TB/DB = 0.2/0.1 AST/ALT = 16/12 ALP 100 A/G = 3.1/4.0 33. 34. U/S abdomen No free fluid AAA 5 cm Can’t seen intimal flap 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. CT SCAN AAA juxtrareal -> bifurcation Size 10*8*4 cm Inflamatory tissue around AAA Intact renal artery Aortic dissection at juxtra renal -> bifurcation Bowel wall thickening at 3 rd -4 th part of duodenum 45. Progress note 09.30 : BP 190/110 , PR 150/min 10.00 : BP 200/120 , PR 136/min 10.30 : BP 262/155 , PR 131/min Start propanolol 40 mg oral & NTG drip Consult med , consult surg 13.45 : BP 126/93 , PR 130 (NTG35ud/min ) 15.30 : CT abdomen with contrast 46. Progress note 15.45 : consult surg ให้ความเห็นว่า น่าจะเป็น chronic dissecting aneurysm ของเก่าอยู่แล้ว ส่วนเรื่อง limb คิดว่าเป็น chronic arterial occlusion ให้ med ดูต่อ และถ้า stable ให้ทำ MRI 16.00 : cardio med : นึกถึง hypertensive emergency with dissecting aneurysm ให้ drip NTG ต่อ และ continue b-blocker 47. 15/02/50 BP 110/70-140/80 (NTG 60 ud/min , herbessor (1:60) 30 ud/min ) PR 80/min Urine 2 ml/kg/hr Cr 0.4 Hct 27 (PRC 2 unit) , no active bleeding 48. 16/02/50 BP 130/80 , PR 70 , RR 18 Hct 31 , no active bleeding Consult surg อีกครั้ง เรื่อง dissecting aneurysm ศัลยกรรมตอนแรก plan ผ่าตัด แต่ต่อมาขอเลื่อน เนื่องจากต้องการรอผล aortogram , CT chest ก่อน 49. 50. 23/02/50 ระหว่างรอทำ CT angiogram ผู้ป่วยอาเจียนเป็นเลือดจำนวนมาก 1 กระโถน BP drop 50/30 , PR 130 ETT , load iv , G/M BP 70/50 หลังได้ iv ~ 5000 ml Set OR emergency 51. 52. 53. 54. 55. 56. 57. 58. Dissecting involve descending aorta splanchnic ischemia Renal failure lower extremity ischemia focal neurologic deficits due to spinal artery involvement spinal cord ischemia 59. 60. 61. 62. 63. Blood pressure control labetalol 0.25 mg/kg iv (or 20 mg) over 2 minutes and then nitroprusside 0.3 to 10 μg/kg/min keep HR 60 – 80 beats/min reduction of systolic blood pressure to 100 to 120 mmHg or the lowest level that is tolerated 64. Indication for surgery Involve aortic root (DeBakey I,II) (standford A) Descending type with complication Rupture Limb ischemia Spinal cord ischemia Renal failure Bowel ischemia Progressive & expansion 65.