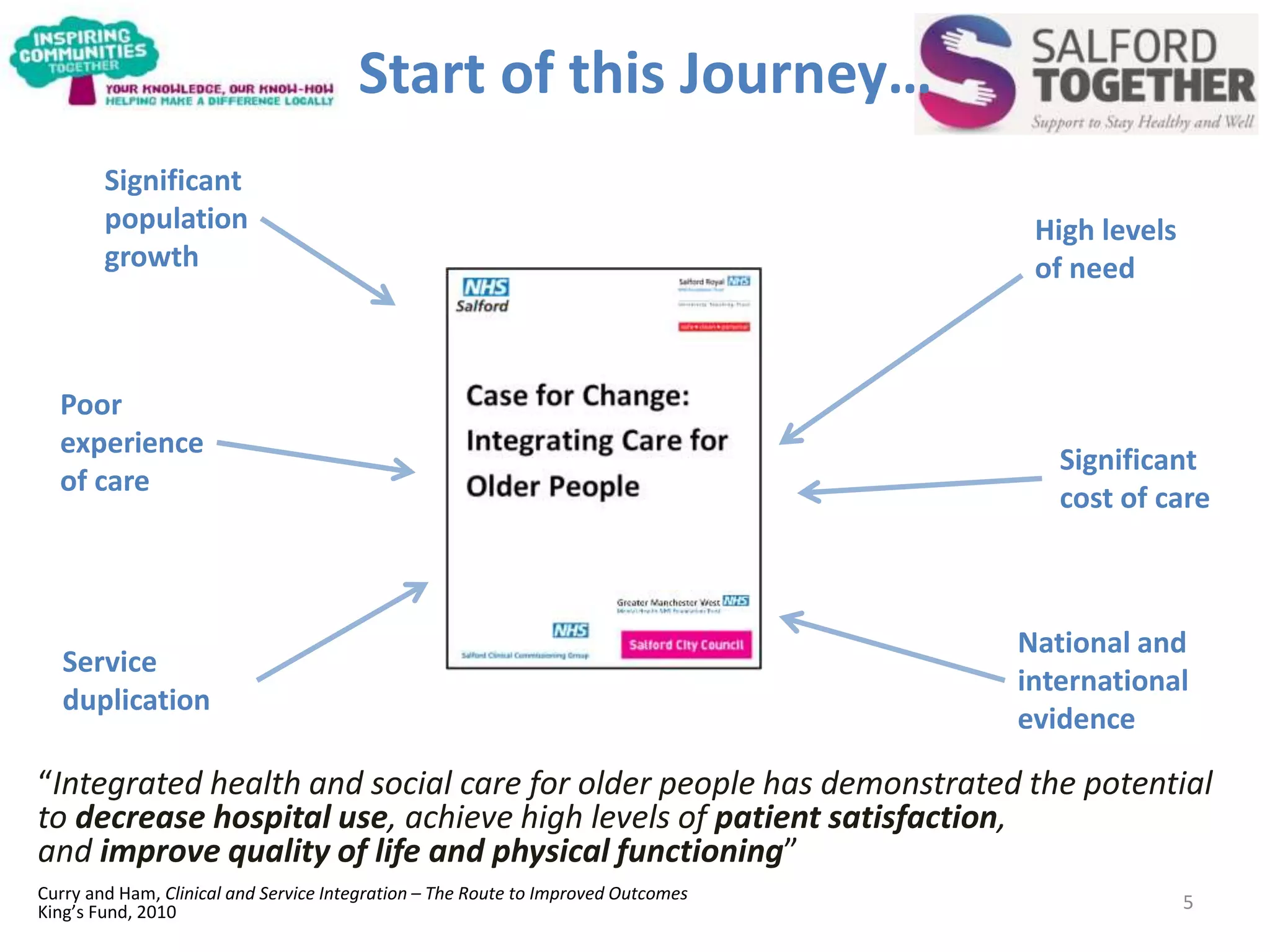
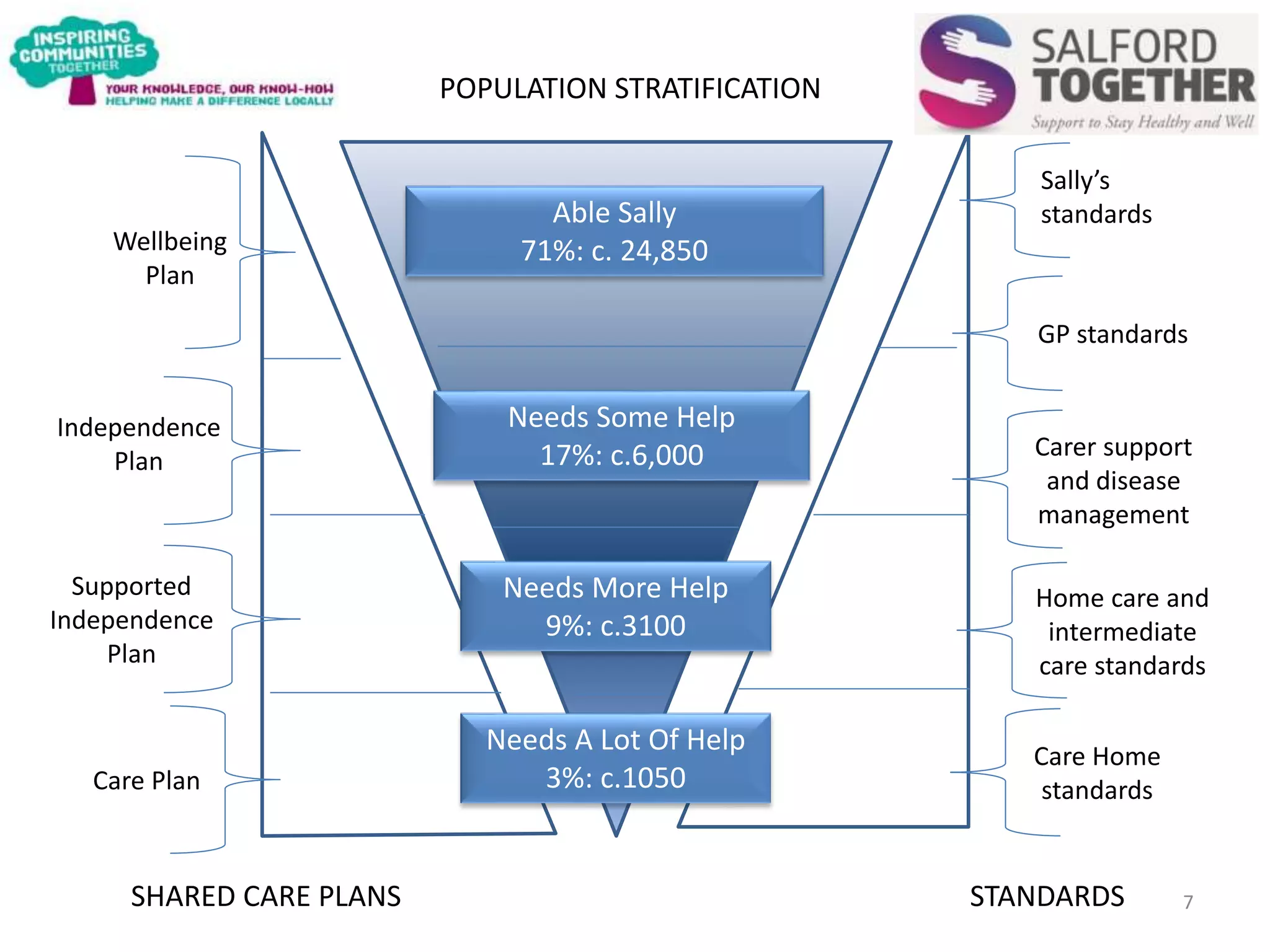
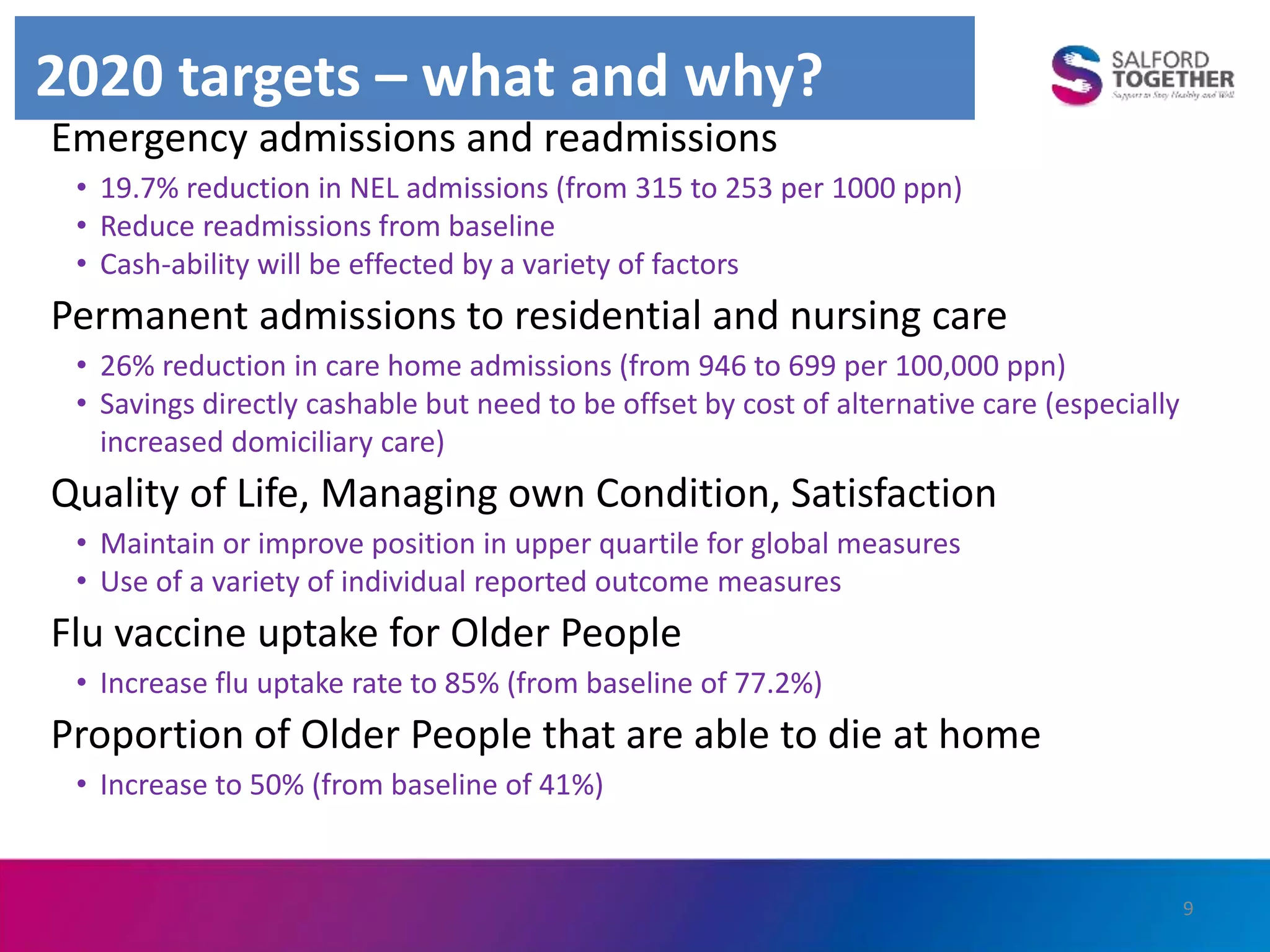
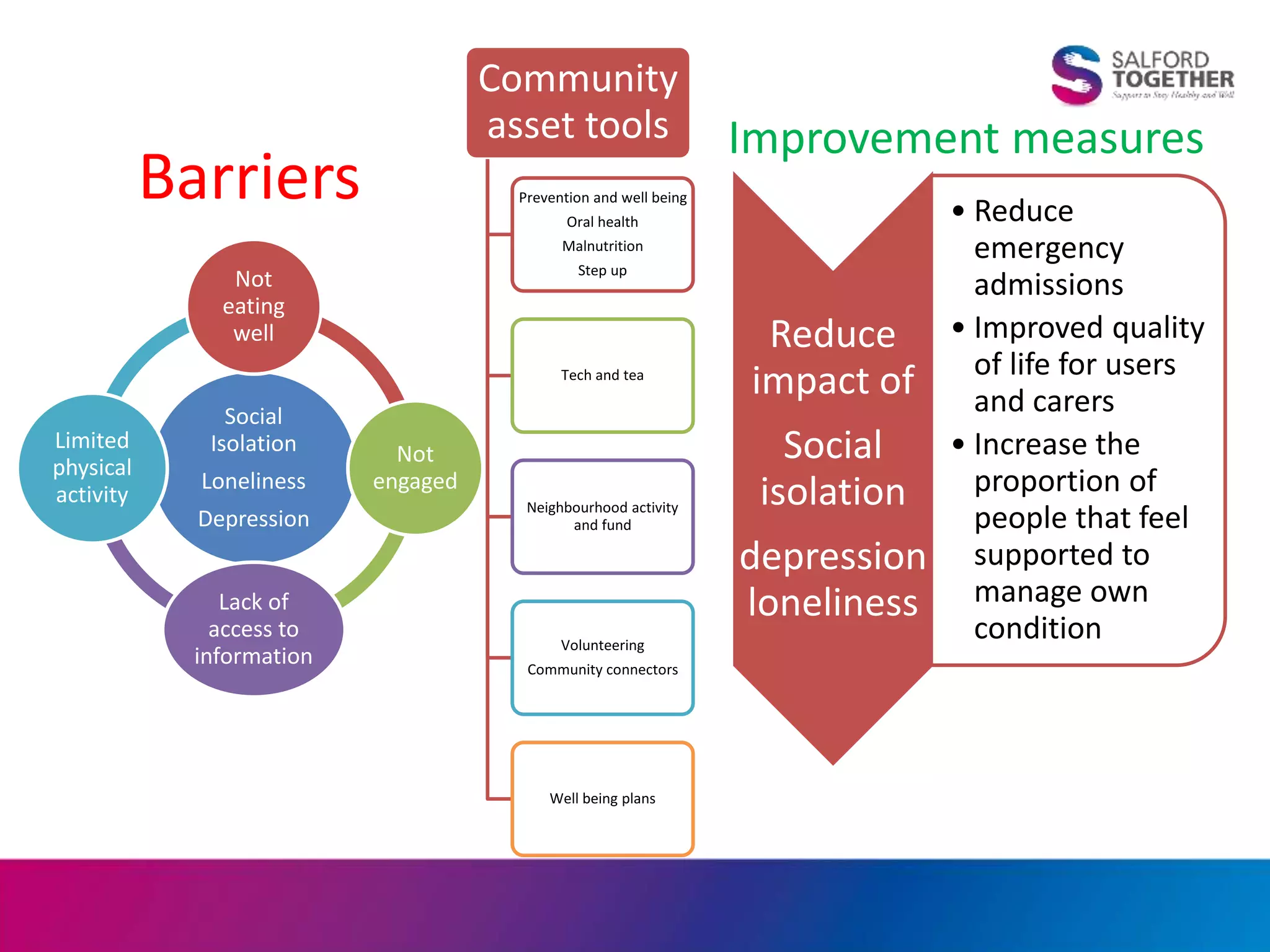
The document discusses Inspiring Communities Together, a neighbourhood charity in Salford, and its strategic context within integrated health and social care. It outlines Salford's integrated care programme which aims to promote independence for older people through a multi-disciplinary approach. Key elements include a Centre of Contact, multi-disciplinary groups, and utilizing local community assets to help older adults remain independent.