INTRODUCTION
• First truebionic sense organs.
• Like human cell, receive mechanical sound energy and convert it into a series of electrical impulses.
• Human cochlea is an electromechanical transducer.
• It has been estimated that only 10% of the normal spiral ganglion cell population of 35,000 is necessary for
successful cochlear implant use.
• The lowest numbers of surviving spiral ganglion cells are seen in individuals with congenital/genetically
mediated losses and following bacterial meningitis.
• A strong positive correlation has seen between the diameter of the cochlear nerve and the total spiral
ganglion cell count
3.
BASIC CONCEPT
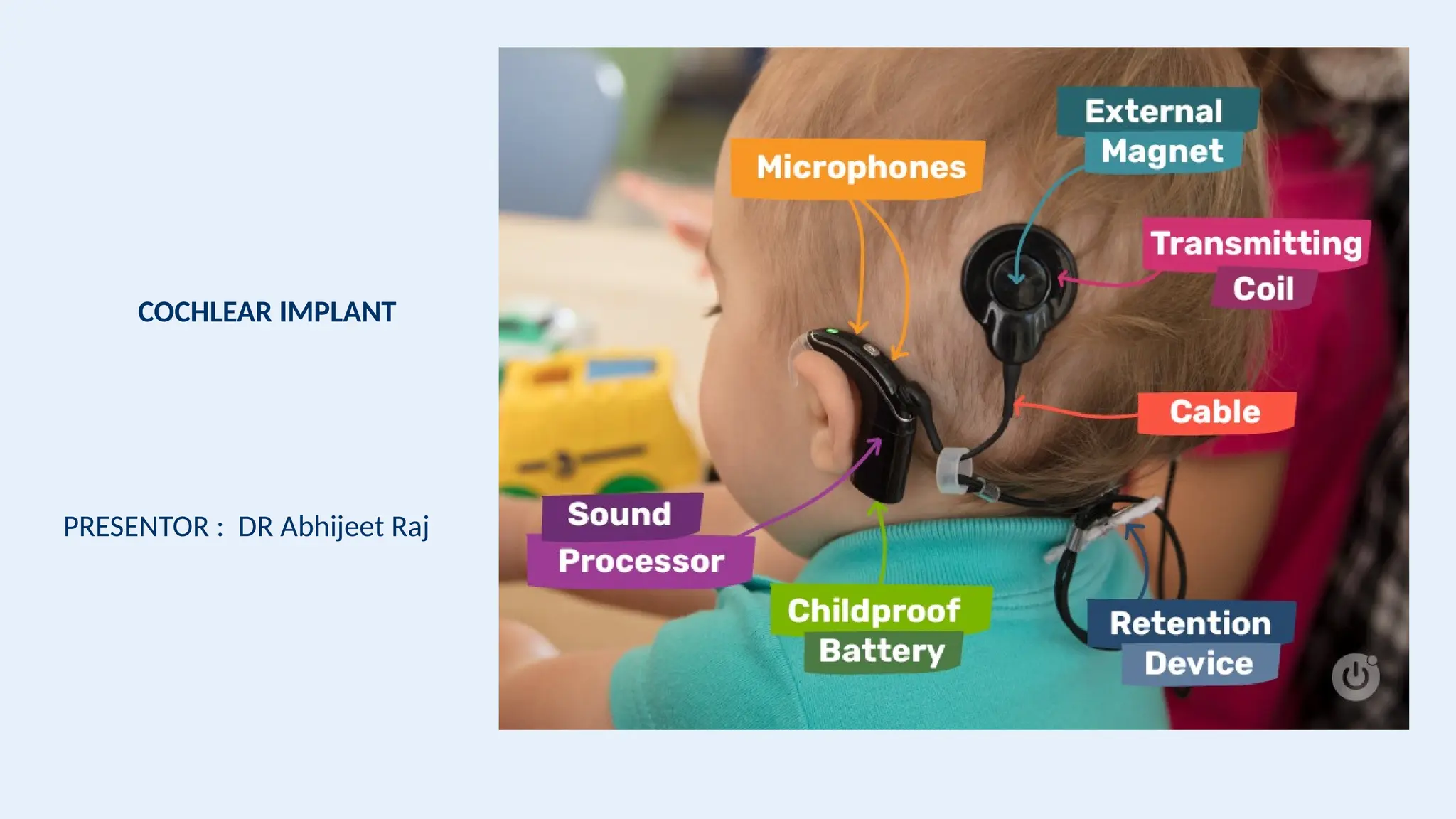
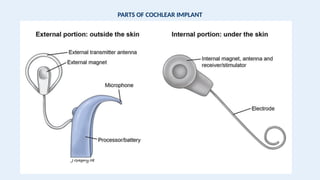
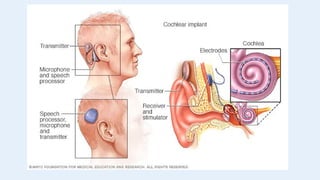
• Acochlear implant consists of external and internal (surgically implanted) components.
• The external components include:
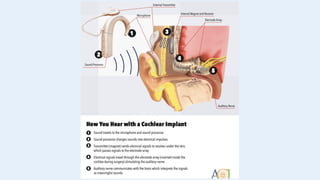
• A microphone that picks up sounds from the environment;
• A speech processor (a computer) that analyzes and digitizes sound signals and sends them to a transmitter
• A transmitter worn on the head that sends the signal to the surgically implanted internal receiver/stimulator.
• The internal components include:
• A receiver/stimulator just under the skin which receives signals from the processor and converts them into
electric impulses
• An electrode array that receives the signal from the transmitter and stimulates the auditory nerve. The
transmitted information is then sent to the brain, which "learns” to interpret the signal as meaningful
information.
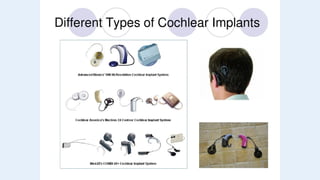
TYPES
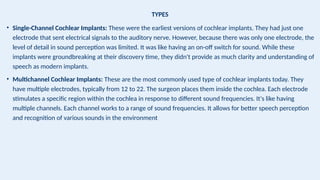
• Single-Channel CochlearImplants: These were the earliest versions of cochlear implants. They had just one
electrode that sent electrical signals to the auditory nerve. However, because there was only one electrode, the
level of detail in sound perception was limited. It was like having an on-off switch for sound. While these
implants were groundbreaking at their discovery time, they didn't provide as much clarity and understanding of
speech as modern implants.
• Multichannel Cochlear Implants: These are the most commonly used type of cochlear implants today. They
have multiple electrodes, typically from 12 to 22. The surgeon places them inside the cochlea. Each electrode
stimulates a specific region within the cochlea in response to different sound frequencies. It's like having
multiple channels. Each channel works to a range of sound frequencies. It allows for better speech perception
and recognition of various sounds in the environment
10.
INDICATIONS
• Children agedbetween 12 and 24 months with profound sensineural hearing loss , children aged between 2
and 17 years with severe to profound SNHL.
• The age of implantation has slowly been lowered from 2 years through 18 months to 1 year of age.
• Adults with moderate to profound SNHL in whom hearing aid are of minimal benefit.
• Candidates must have both the absence of a central auditory lesion and the presence of an auditory nerve
confirmed radiographically during their workup.
14.
PRE OPERATIVE EVALUATION
•Objective testing in a child should include tympanometry, diagnostic auditory brainstem testing, and
otoacoustic emission assessment.
15.
PRE OPERATIVE EVALUATION
•Initial screening for cochlear implant candidacy in postlingually deafened adults begins with pure-tone
audiometry and speech discrimination testing.
• As a general rule, potential cochlear implant candidates will have a pure tone average greater than 50 dB
and a standard speech discrimination score of less than 50 to 60%.
• Final candidacy determination be made using Hearing in Noise Test (HINT) sentence testing and
consonant/nucleus/consonant (CNC) word testing.
• Hearing in Noise Test sentence scores of less than 50% in quiet and CNC scores of less than 30% are used as
general candidacy guidelines.
16.
PRE OPERATIVE EVALUATION
•The Early Speech Perception (ESP) test assesses speech perception ability and is available in both a low
verbal and a standard version. Speech perception ability is divided into three subtests to assess the child’s
capacity to
• (1) distinguish patterns in speech (“ball” versus “cookie” versus “airplane” versus “ice cream cone”)
• (2) identify spondee words (“hot dog,” “cowboy,” “airplane”)
• (3) to discriminate monosyllabic words (“ball”,“boot”, “boat”, “bat”). It is useful for children who have
developed some language skills.
17.
MEDICAL EVALUATION
• Onceit has been determined that a person is a good audiologic candidate, a medical evaluation is necessary.
The medical evaluation should determine that a candidate can undergo the operative procedure with
acceptable risks.
• Radiographic imaging of the temporal bone should be obtained in order to identify any potential anatomic
variations that might contraindicate the operation or require alterations to the usual surgical procedure.
19.
• Normal anatomyof Inner Ear
structures in high-resolution CT
(selection of 0.625-mm thick axial
slices); caudocranial direction
from a to d. Legend: ATC: apical
turn cochlea; BTC: basal turn
cochlea; MTC: middle turn
cochlea; CA: cochlear aqueduct;
ET: eustachian tube (entrance);
IAC: internal auditory canal; ICA:
internal carotid artery; M:
malleus; LSCC: lateral semicircular
canal; PSCC: posterior
semicircular canal; SSCC: superior
semicircular canal; V: vestibule;
VA: vestibular aqueduct; VII: 7th
cranial nerve (LS: labyrinthine
segment; MS: mastoid segment;
TS: tympanic segment); GG:
geniculate ganglion
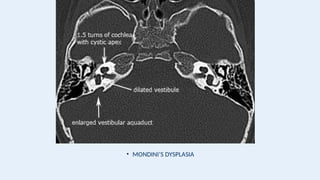
20.
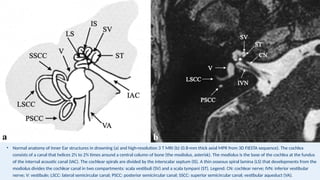
• Normal anatomyof Inner Ear structures in drowning (a) and high-resolution 3 T MRI (b) (0.8-mm thick axial MPR from 3D FIESTA sequence). The cochlea
consists of a canal that helices 2½ to 2¾ times around a central column of bone (the modiolus, asterisk). The modiolus is the base of the cochlea at the fundus
of the internal acoustic canal (IAC). The cochlear spirals are divided by the interscalar septum (IS). A thin osseous spiral lamina (LS) that developments from the
modiolus divides the cochlear canal in two compartments: scala vestibuli (SV) and a scala tympani (ST). Legend: CN: cochlear nerve; IVN: inferior vestibular
nerve; V: vestibule; LSCC: lateral semicircular canal; PSCC: posterior semicircular canal; SSCC: superior semicircular canal; vestibular aqueduct (VA).
21.
• It hasbecome clear that MRI is the most sensitive technique for identifying early labyrinthitis
ossificans.
• Even high- resolution CT scanning may miss cochlear obstruction in up to 50% of candidates.
• Computed tomographic scanning cannot detect labyrinthine obstruction until frank ossification
has developed.
• On the other hand, MRI relies on the presence or absence of a fluid signal within the
labyrinthine bone.
22.
• MRI hasbecome the diagnostic modality of choice for the detection of postmeningitic
endocochlear obstruction.
• Magnetic resonance imaging can demonstrate an absent or hypoplastic cochlear nerve.
• Defects in the cribriform area of the cochlea, which present the likelihood of an intraoperative
“gusher,” can be identified on MRI scanning and warn the surgeon about this potential difficulty.
• High-resolution CT scanning, however, permits more complete characterization of hypoplasia,
aplasia, and incomplete partitioning defects (eg, the Modini deformity).
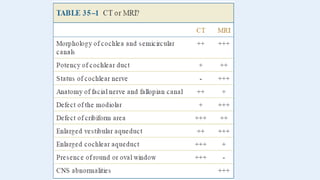
WHICH EAR HASTO BE IMPLANTED
• In the earliest days of cochlear implantation, the worse hearing ear was generally selected. It
was argued that the implantation itself would destroy residual hearing (and it does in at least 50
% of cases) and that the better hearing ear should be conserved in case the implant did not
work.
• Consequently, many programs currently select the better hearing ear. It is reasoned that the
better hearing ear is likely to have a higher population of residual neural elements and hence
offer the possibility of better performance.
• The most recently deafened ear is chosen.
25.
• Anatomic considerationsmay guide side selection. If one ear is significantly dysplastic or hypoplastic,
the contralateral ear may be selected.
• While long-standing labyrinthitis ossificans is generally symmetric, initially it may progress more rapidly
in one ear than in the other. The least obstructed labyrinth should be chosen.
• Canal wall down mastoidectomy in one ear would make the contralateral side more appealing because
the standard operative procedure would not require modification.
• Previous trauma (surgical or otherwise) may have significantly reduced labyrinthine function on one
side.
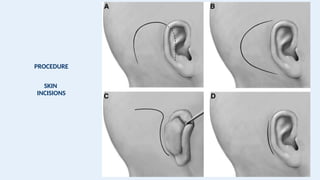
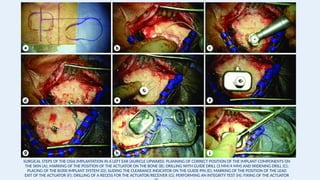
SURGICAL STEPS OFTHE OSIA IMPLANTATION IN A LEFT EAR (AURICLE UPWARD): PLANNING OF CORRECT POSITION OF THE IMPLANT COMPONENTS ON
THE SKIN (A); MARKING OF THE POSITION OF THE ACTUATOR ON THE BONE (B); DRILLING WITH GUIDE DRILL (3 MM/4 MM) AND WIDENING DRILL (C);
PLACING OF THE BI300 IMPLANT SYSTEM (D); SLIDING THE CLEARANCE INDICATOR ON THE GUIDE PIN (E); MARKING OF THE POSITION OF THE LEAD
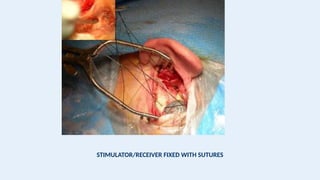
EXIT OF THE ACTUATOR (F); DRILLING OF A RECESS FOR THE ACTUATOR/RECEIVER (G); PERFORMING AN INTEGRITY TEST (H); FIXING OF THE ACTUATOR
REVISION SURGERY
• Thereare several reasons for reoperating in the area of an existing cochlear implant:
• 1. There has been device failure.
• 2. A technologically outdated device needs to be removed and an updated device inserted.
• 3. The device becomes extruded or exposed. Revision operation may or may not require explantation
and/or reimplantation.
• 4. The skin flap must be revised, usually because it is too thick.
• 5. An additional procedure is being performed in the area of the implant eg, auricular reconstruction.
POSTOPERATIVE CONSIDERATIONS FORSURGEONS
• Device activation - Two to four weeks postoperatively, when the wound is well healed, the
cochlear implant is activated. This is a process frequently referred to as “hook up.”
• Facial Nerve Stimulation.
• Postoperative rehabilitation.
• Speech and Language Aquisition - Cochlear implants, in summary, allow a child to recover a
normal ability to acquire speech and language once the implant has been placed but do not
fully overcome the detrimental effects of early auditory deprivation. Thus, the gap between
chronological age and language age, which progressively increases in unimplanted children,
remains constant after cochlear implantation.









![cochlear implant [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cochlearimplantautosaved-230807191245-e9fc2957-thumbnail.jpg?width=640&height=640&fit=bounds)



















![Recent_Advances_Cochlear_Implant_Candidacy_Dr_Anand_Gupta[1]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancescochlearimplantcandidacydranandgupta1-1-251128040227-e519dadb-thumbnail.jpg?width=640&height=640&fit=bounds)






















