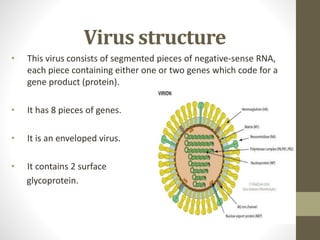
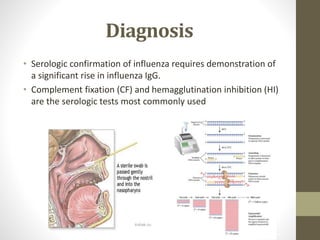
This document provides an overview of influenza viruses including etiology, structure, types (A, B, C), antigenic shift and drift, pathogenesis, clinical features, transmission, epidemiology, diagnosis, treatment and prevention with vaccines. It describes how influenza A viruses are classified into subtypes based on surface proteins and how antigenic shift and drift allow new strains to evade immunity. It also summarizes influenza virus structure, the RNA segments that encode proteins, and the two surface glycoproteins. Complications, diagnostic methods, antiviral treatments, vaccine history and effectiveness are briefly outlined.