![Evidence:
1. Rubio et al. (2014)
9.7% increase in CPR compared to traditional
culture and morphology assessments alone.
2. Cochrane review, Armstrong et al., 2015
insufficient evidence of differences in live birth,
miscarriage, stillbirth or clinical pregnancy to
choose between [TL imaging] and conventional
incubation
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/labadjuvant-170621061855/85/Adjuncts-in-IVF-laboratory-Current-evidence-15-320.jpg)
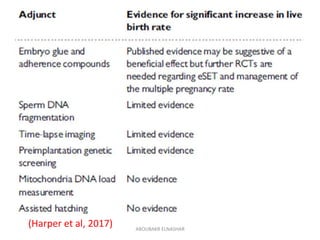

This document summarizes several adjunct techniques used in IVF laboratories including sperm DNA fragmentation testing, advanced sperm selection methods like IMSI and pICSI, embryo selection techniques like time-lapse imaging and PGS, and mitochondrial DNA load measurement. It reviews the current evidence for each technique, noting that while some like TL imaging show promise, the evidence is still limited and inconclusive for many techniques to recommend their routine use to improve IVF outcomes. Larger randomized controlled trials are still needed to prove effectiveness.























































































