Download to read offline

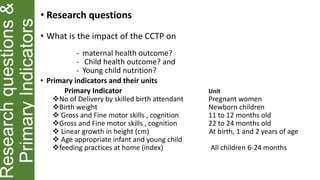
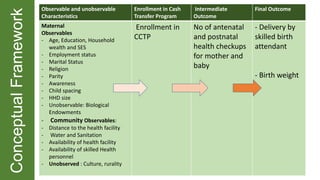
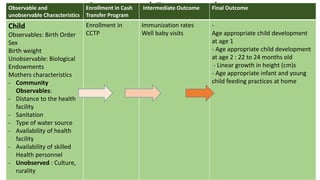
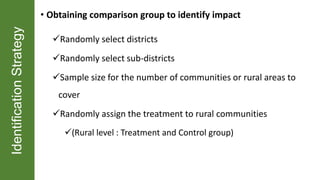
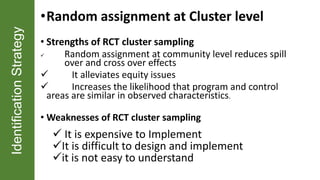
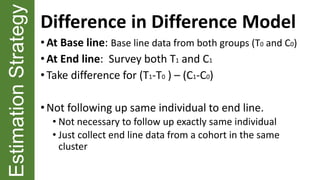

The document outlines a Conditional Cash Transfer Program (CCTP) in rural China aimed at improving maternal and child health outcomes through monthly cash transfers tied to health facility utilization. It discusses the program's objectives, eligibility criteria, research questions, indicators, and evaluation strategies over a three-year period, including a random assignment for comparison. The program aims to enhance maternal and child health by increasing the use of public health facilities and covering key indicators such as delivery by skilled attendants and child nutrition.




















































































