Download to read offline
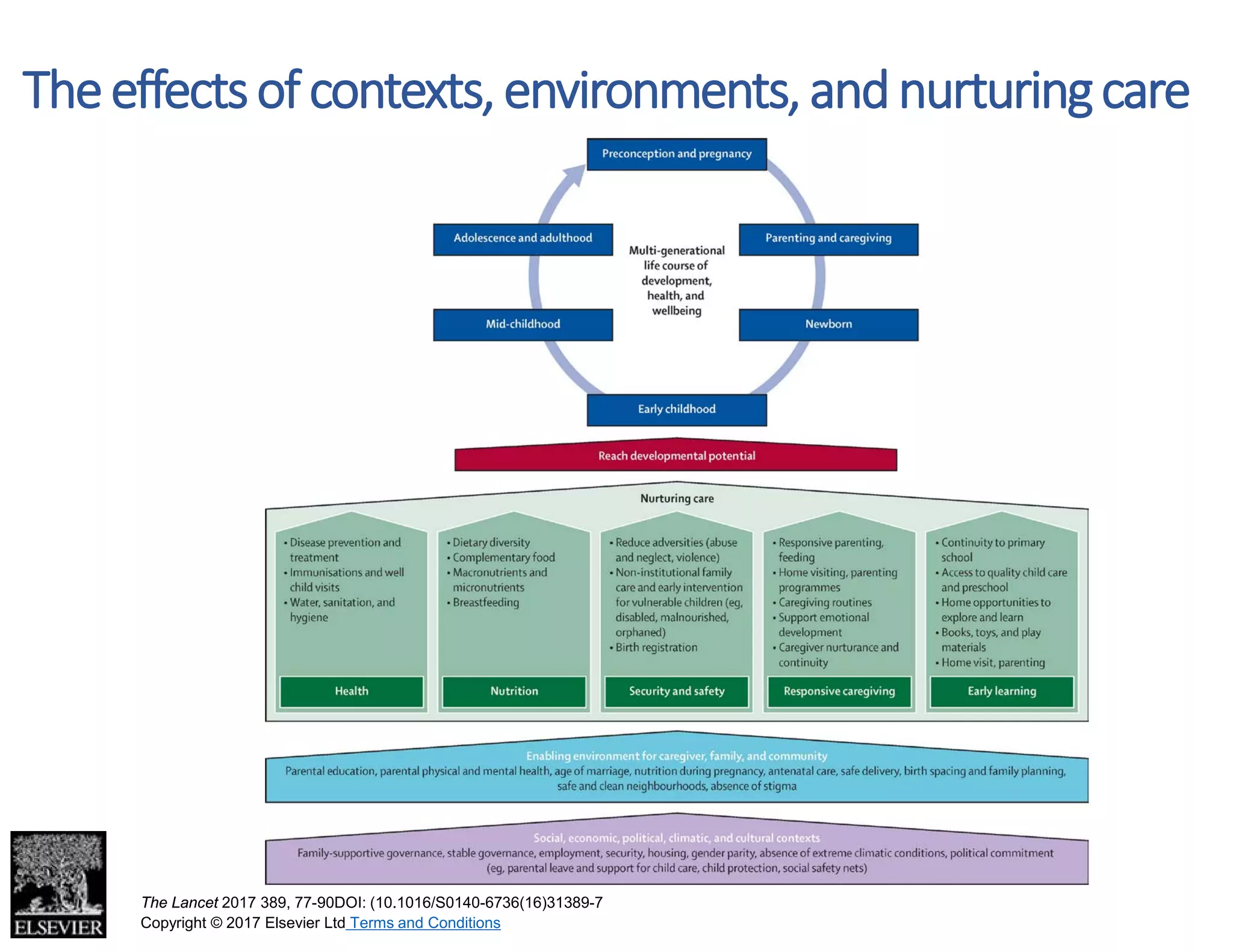
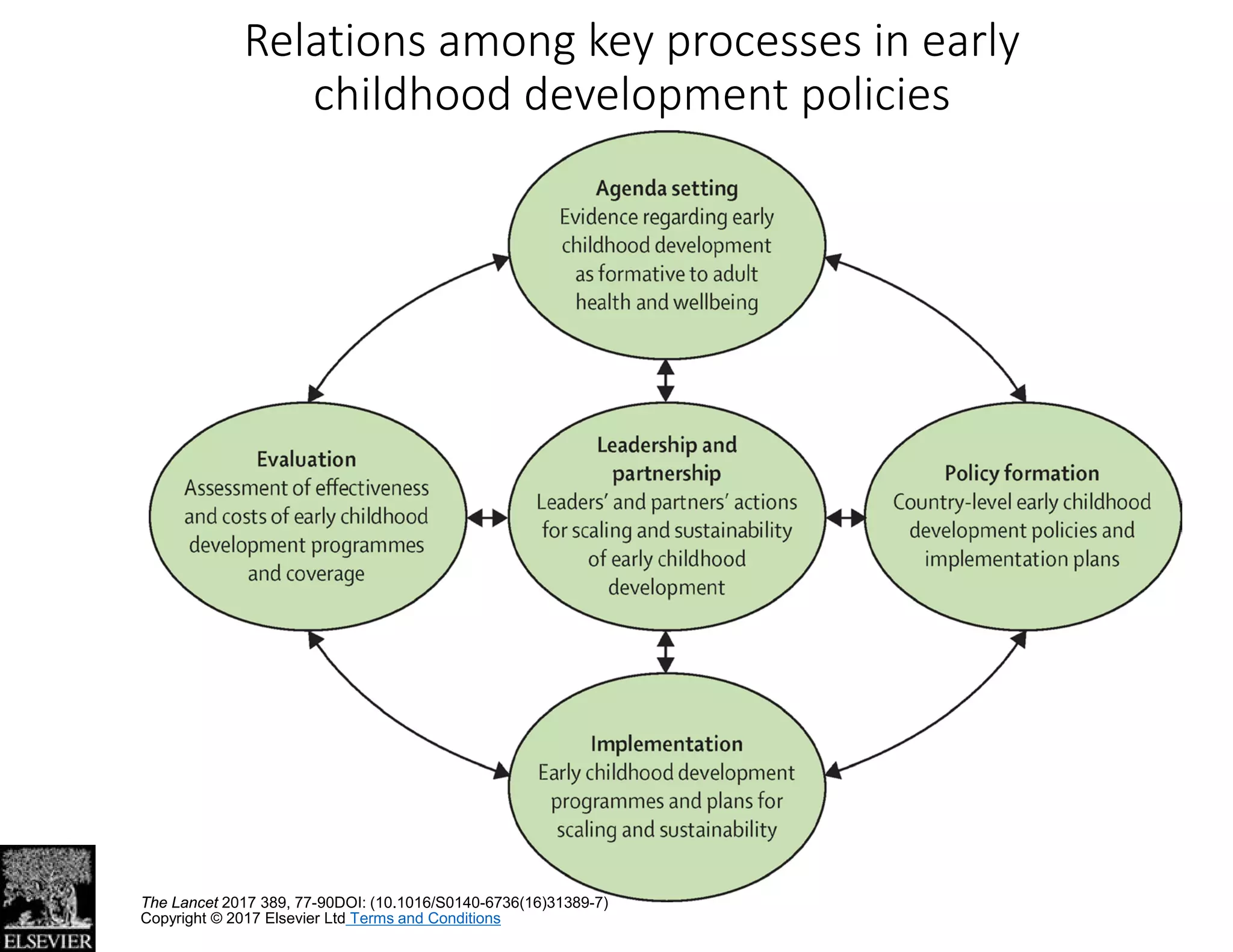

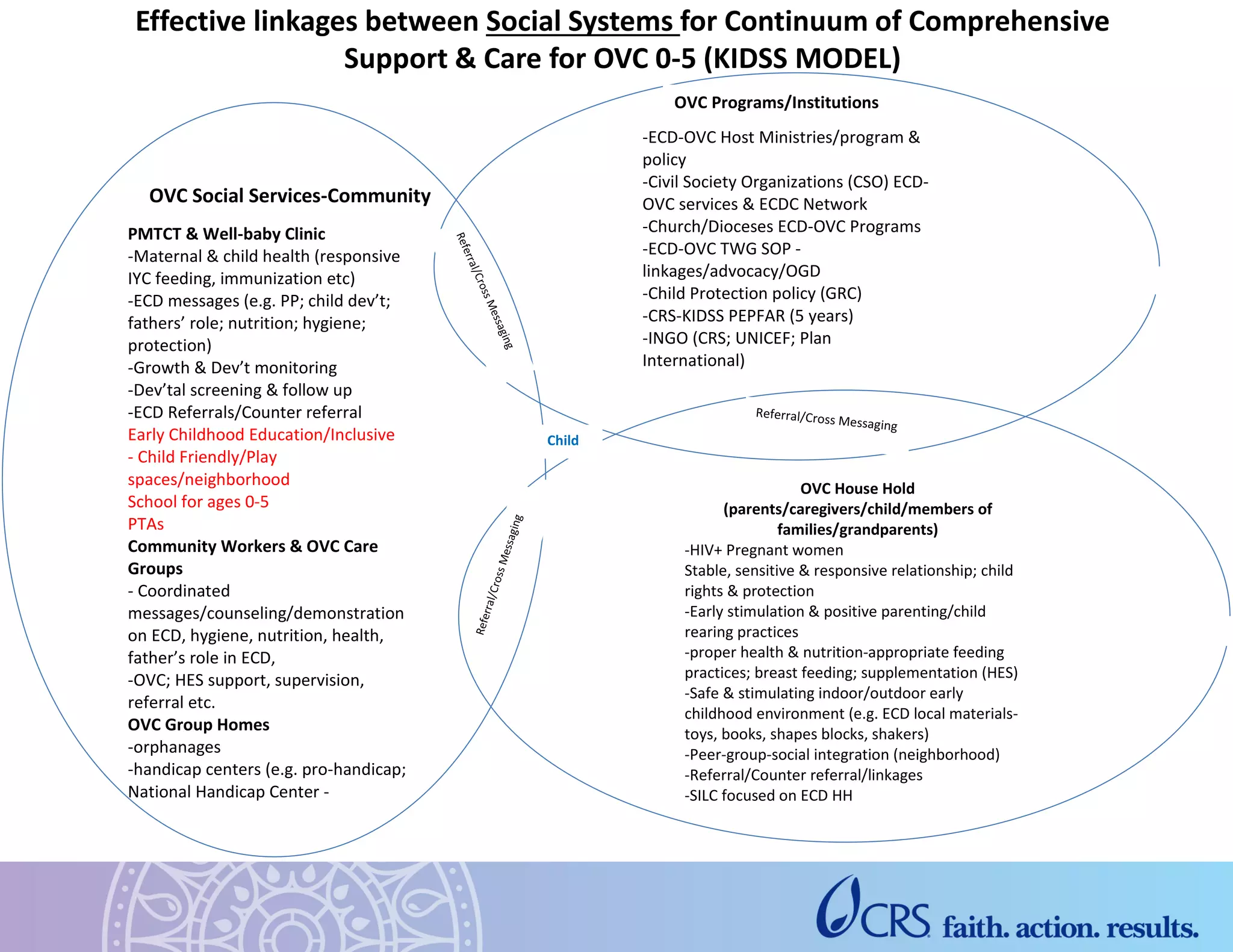
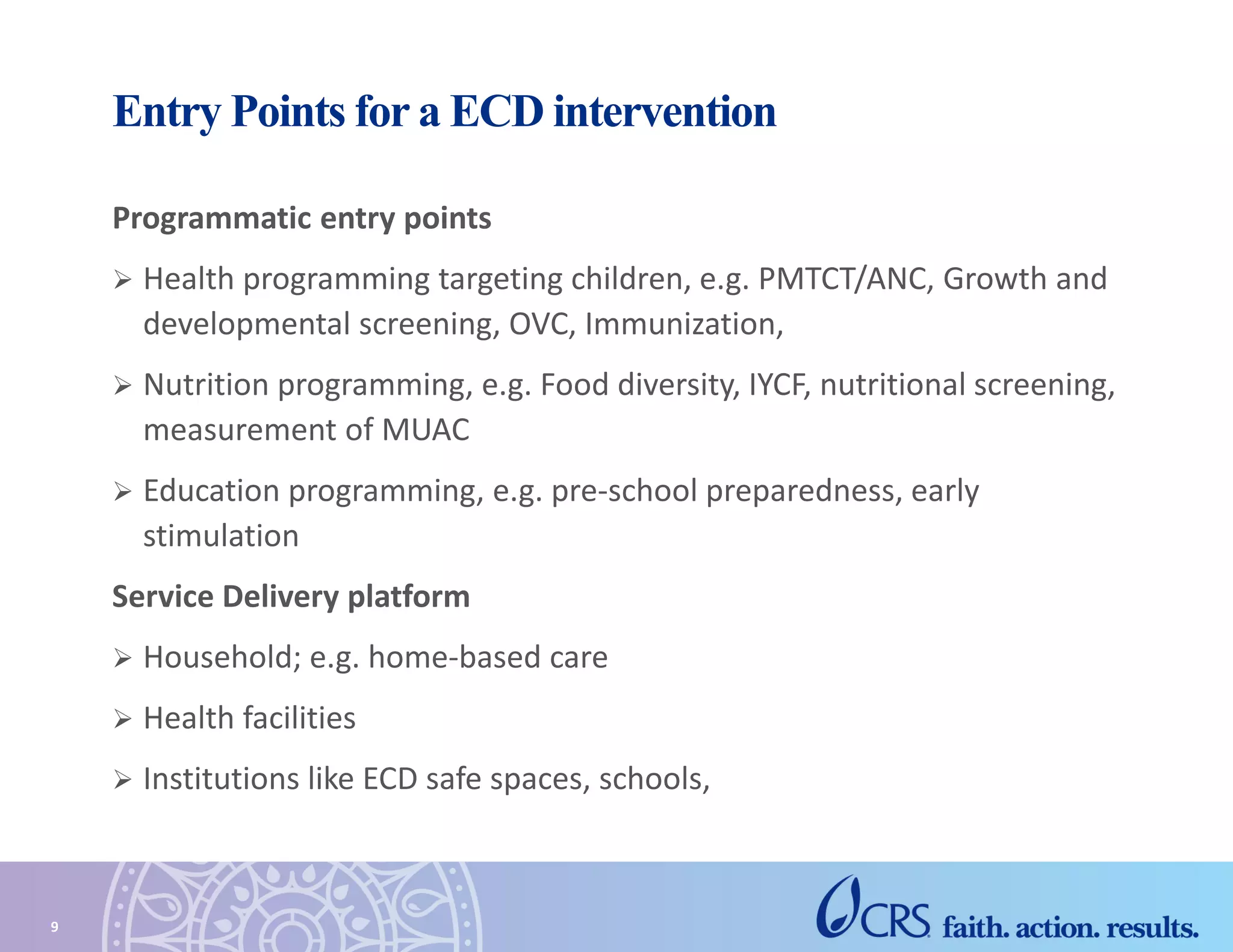


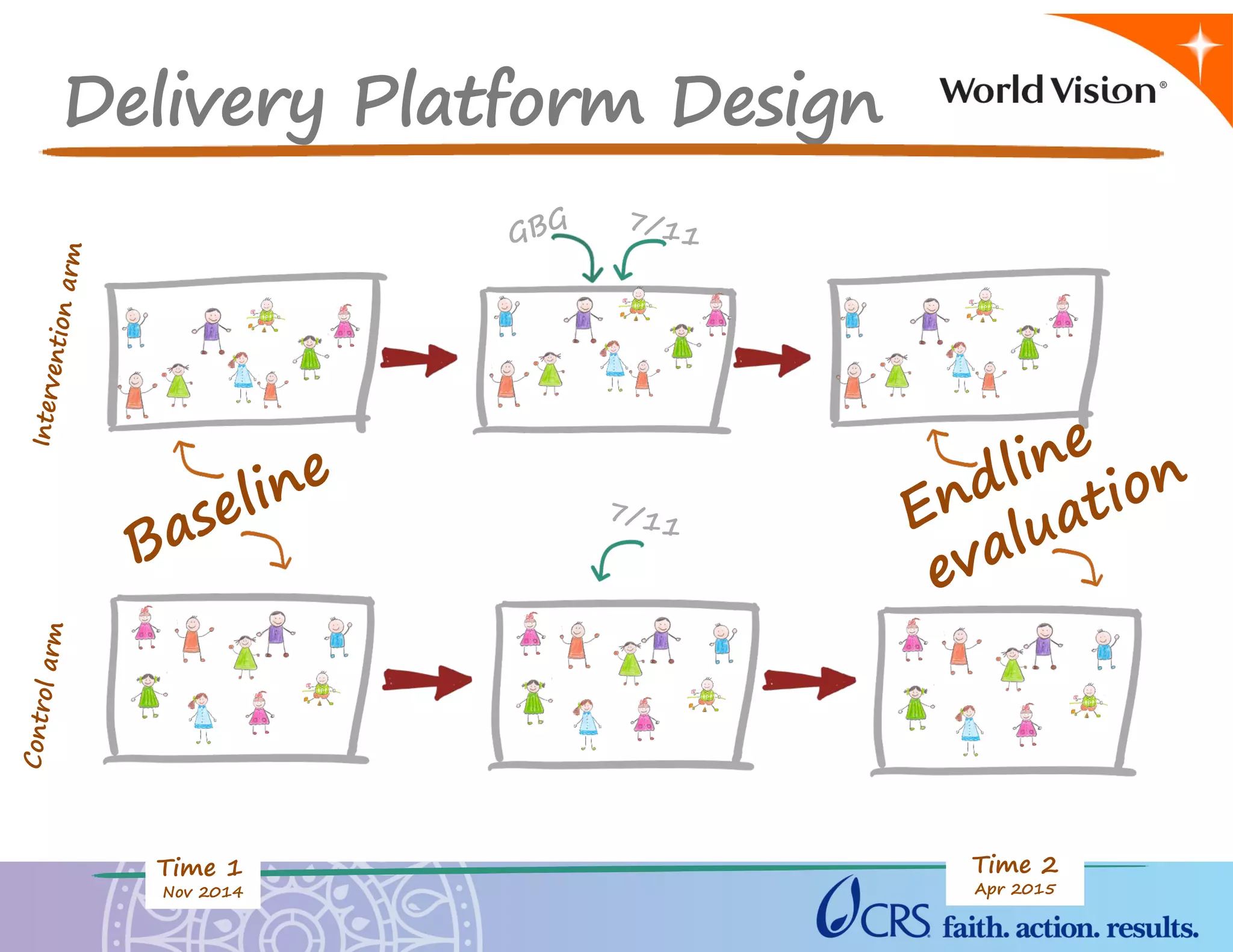





The document discusses early childhood development programs in various countries, highlighting strategies for implementation and evaluation of such programs. It also reviews evidence from The Lancet series on the importance of early childhood development and the impact of adverse and positive experiences on brain development. Examples are provided of early childhood development best practices and gaps within the KIDSS project in addressing health, nutrition, and educational needs of young children.










































































