Download to read offline



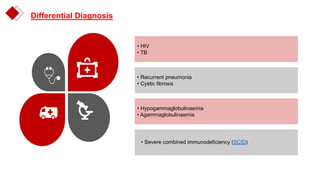





A 4-year old girl presented with recurrent anaemia, rash, hepatosplenomegaly, and failure to thrive. Examinations found dysmorphic features, lymphadenopathy, and delayed development. Investigations showed pneumonitis, skin inflammation, liver granuloma, and bone marrow fibrosis. T- and B-cell lypopaenia suggested primary immunodeficiency, likely severe combined immunodeficiency (SCID). She received transfusions, antibiotics, antituberculosis treatment, and IV immunoglobulin. Bone marrow transplant is the cure for SCID but she was lost to follow up after discharge.





































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)













