
Downloaded 257 times












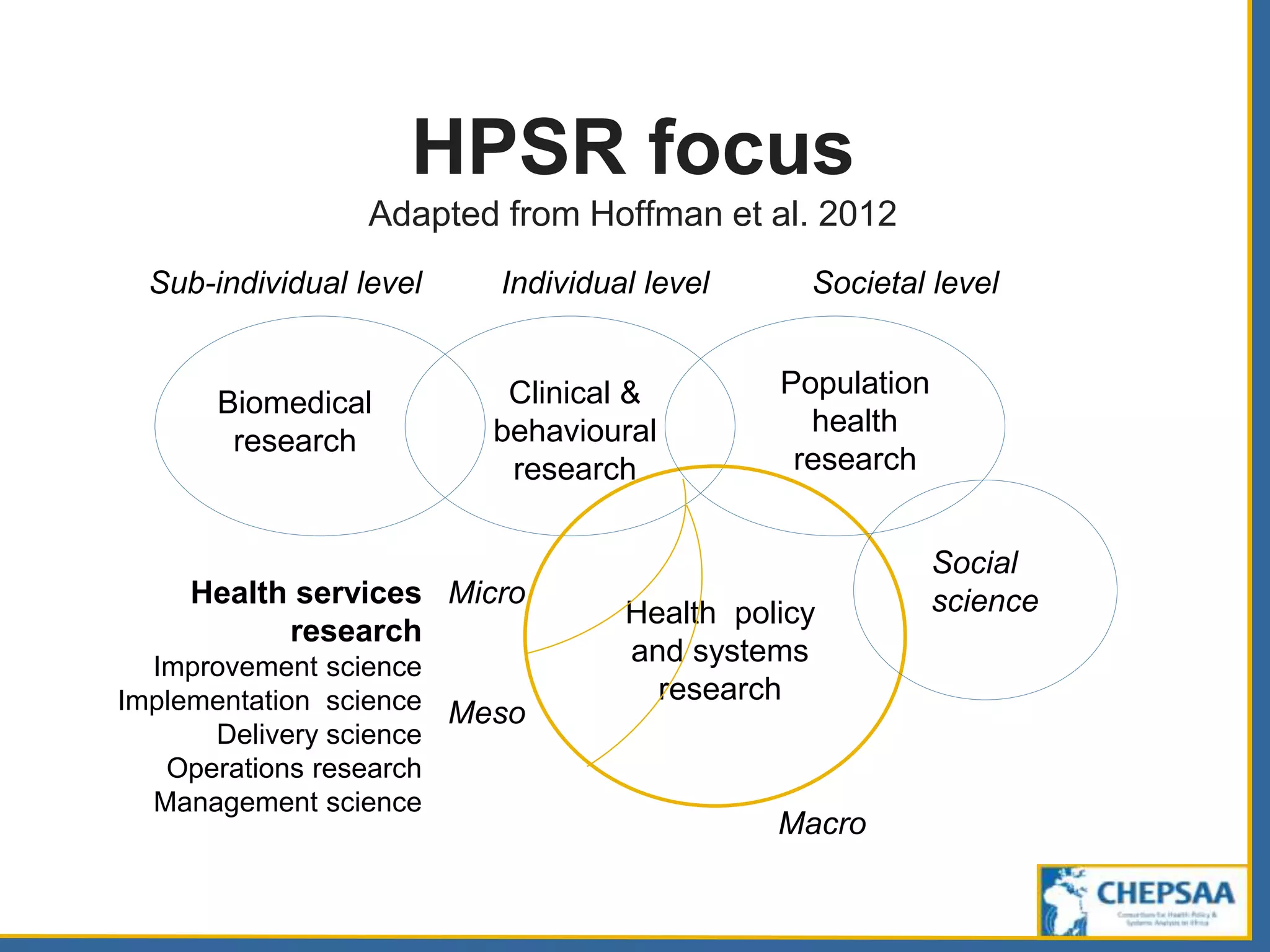










HPSR stands for health policy and systems research. It seeks to understand how societies organize themselves to achieve health goals and how different actors interact in the policy and implementation processes to contribute to health outcomes. It is interdisciplinary, drawing from fields like economics, sociology, and public health. HPSR is distinguished by the issues and questions considered rather than disciplinary base. It focuses on both describing health systems and evaluating them, as well as analyzing policies and the policy-making process. The research considers multiple levels from macro to micro. A range of study designs can be used depending on the question.





























































































